Lies Langouche, Arno Téblick, Jan Gunst, Greet Van den Berghe
{"title":"下丘脑-垂体-肾上腺皮质对危重疾病的反应:一个需要修正的概念。","authors":"Lies Langouche, Arno Téblick, Jan Gunst, Greet Van den Berghe","doi":"10.1210/endrev/bnad021","DOIUrl":null,"url":null,"abstract":"<p><p>Based on insights obtained during the past decade, the classical concept of an activated hypothalamus-pituitary-adrenocortical axis in response to critical illness is in need of revision. After a brief central hypothalamus-pituitary-adrenocortical axis activation, the vital maintenance of increased systemic cortisol availability and action in response to critical illness is predominantly driven by peripheral adaptations rather than by an ongoing centrally activated several-fold increased production and secretion of cortisol. Besides the known reduction of cortisol-binding proteins that increases free cortisol, these peripheral responses comprise suppressed cortisol metabolism in liver and kidney, prolonging cortisol half-life, and local alterations in expression of 11βHSD1, glucocorticoid receptor-α (GRα), and FK506 binding protein 5 (FKBP51) that appear to titrate increased GRα action in vital organs and tissues while reducing GRα action in neutrophils, possibly preventing immune-suppressive off-target effects of increased systemic cortisol availability. Peripherally increased cortisol exerts negative feed-back inhibition at the pituitary level impairing processing of pro-opiomelanocortin into ACTH, thereby reducing ACTH-driven cortisol secretion, whereas ongoing central activation results in increased circulating pro-opiomelanocortin. These alterations seem adaptive and beneficial for the host in the short term. However, as a consequence, patients with prolonged critical illness who require intensive care for weeks or longer may develop a form of central adrenal insufficiency. The new findings supersede earlier concepts such as \"relative,\" as opposed to \"absolute,\" adrenal insufficiency and generalized systemic glucocorticoid resistance in the critically ill. The findings also question the scientific basis for broad implementation of stress dose hydrocortisone treatment of patients suffering from acute septic shock solely based on assumption of cortisol insufficiency.</p>","PeriodicalId":11544,"journal":{"name":"Endocrine reviews","volume":" ","pages":"1096-1106"},"PeriodicalIF":22.0000,"publicationDate":"2023-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10638597/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Hypothalamus-pituitary-adrenocortical Response to Critical Illness: A Concept in Need of Revision.\",\"authors\":\"Lies Langouche, Arno Téblick, Jan Gunst, Greet Van den Berghe\",\"doi\":\"10.1210/endrev/bnad021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Based on insights obtained during the past decade, the classical concept of an activated hypothalamus-pituitary-adrenocortical axis in response to critical illness is in need of revision. After a brief central hypothalamus-pituitary-adrenocortical axis activation, the vital maintenance of increased systemic cortisol availability and action in response to critical illness is predominantly driven by peripheral adaptations rather than by an ongoing centrally activated several-fold increased production and secretion of cortisol. Besides the known reduction of cortisol-binding proteins that increases free cortisol, these peripheral responses comprise suppressed cortisol metabolism in liver and kidney, prolonging cortisol half-life, and local alterations in expression of 11βHSD1, glucocorticoid receptor-α (GRα), and FK506 binding protein 5 (FKBP51) that appear to titrate increased GRα action in vital organs and tissues while reducing GRα action in neutrophils, possibly preventing immune-suppressive off-target effects of increased systemic cortisol availability. Peripherally increased cortisol exerts negative feed-back inhibition at the pituitary level impairing processing of pro-opiomelanocortin into ACTH, thereby reducing ACTH-driven cortisol secretion, whereas ongoing central activation results in increased circulating pro-opiomelanocortin. These alterations seem adaptive and beneficial for the host in the short term. However, as a consequence, patients with prolonged critical illness who require intensive care for weeks or longer may develop a form of central adrenal insufficiency. The new findings supersede earlier concepts such as \\\"relative,\\\" as opposed to \\\"absolute,\\\" adrenal insufficiency and generalized systemic glucocorticoid resistance in the critically ill. The findings also question the scientific basis for broad implementation of stress dose hydrocortisone treatment of patients suffering from acute septic shock solely based on assumption of cortisol insufficiency.</p>\",\"PeriodicalId\":11544,\"journal\":{\"name\":\"Endocrine reviews\",\"volume\":\" \",\"pages\":\"1096-1106\"},\"PeriodicalIF\":22.0000,\"publicationDate\":\"2023-11-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10638597/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1210/endrev/bnad021\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1210/endrev/bnad021","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
The Hypothalamus-pituitary-adrenocortical Response to Critical Illness: A Concept in Need of Revision.
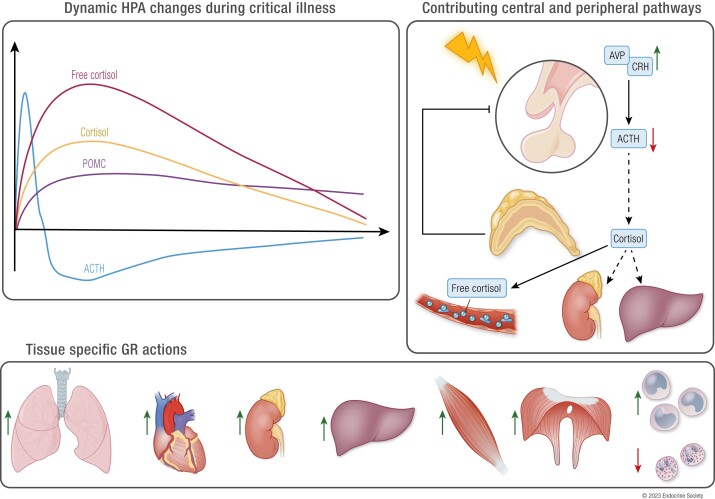
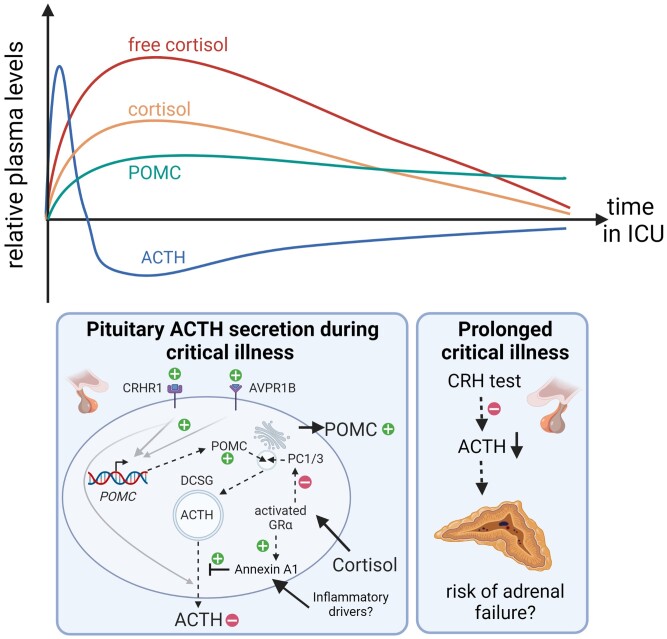
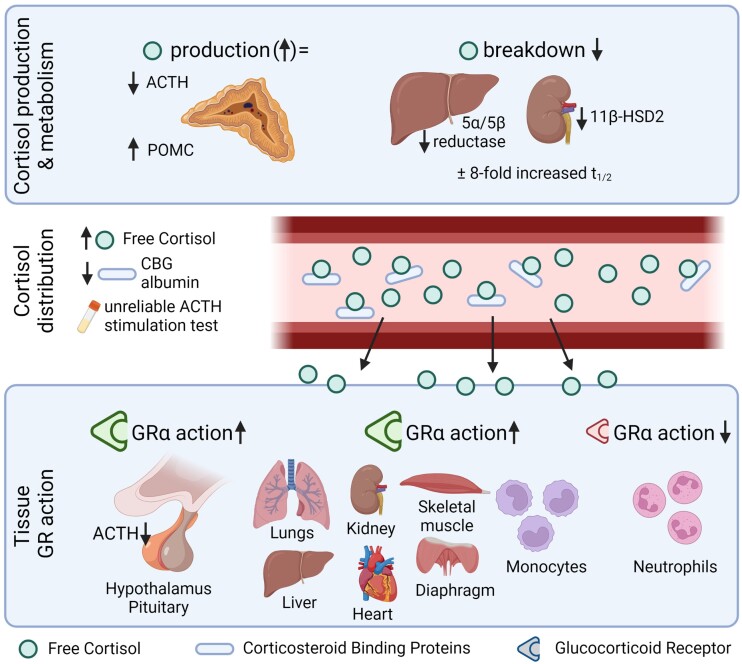
Based on insights obtained during the past decade, the classical concept of an activated hypothalamus-pituitary-adrenocortical axis in response to critical illness is in need of revision. After a brief central hypothalamus-pituitary-adrenocortical axis activation, the vital maintenance of increased systemic cortisol availability and action in response to critical illness is predominantly driven by peripheral adaptations rather than by an ongoing centrally activated several-fold increased production and secretion of cortisol. Besides the known reduction of cortisol-binding proteins that increases free cortisol, these peripheral responses comprise suppressed cortisol metabolism in liver and kidney, prolonging cortisol half-life, and local alterations in expression of 11βHSD1, glucocorticoid receptor-α (GRα), and FK506 binding protein 5 (FKBP51) that appear to titrate increased GRα action in vital organs and tissues while reducing GRα action in neutrophils, possibly preventing immune-suppressive off-target effects of increased systemic cortisol availability. Peripherally increased cortisol exerts negative feed-back inhibition at the pituitary level impairing processing of pro-opiomelanocortin into ACTH, thereby reducing ACTH-driven cortisol secretion, whereas ongoing central activation results in increased circulating pro-opiomelanocortin. These alterations seem adaptive and beneficial for the host in the short term. However, as a consequence, patients with prolonged critical illness who require intensive care for weeks or longer may develop a form of central adrenal insufficiency. The new findings supersede earlier concepts such as "relative," as opposed to "absolute," adrenal insufficiency and generalized systemic glucocorticoid resistance in the critically ill. The findings also question the scientific basis for broad implementation of stress dose hydrocortisone treatment of patients suffering from acute septic shock solely based on assumption of cortisol insufficiency.
期刊介绍:
Endocrine Reviews, published bimonthly, features concise timely reviews updating key mechanistic and clinical concepts, alongside comprehensive, authoritative articles covering both experimental and clinical endocrinology themes. The journal considers topics informing clinical practice based on emerging and established evidence from clinical research. It also reviews advances in endocrine science stemming from studies in cell biology, immunology, pharmacology, genetics, molecular biology, neuroscience, reproductive medicine, and pediatric endocrinology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
