Laurien K L Dhaenens-Meyer, Elisabeth Schriewer, Yvonne G Weber, Stefan Wolking
{"title":"视频脑电图监测以指导抗癫痫药物的停药。","authors":"Laurien K L Dhaenens-Meyer, Elisabeth Schriewer, Yvonne G Weber, Stefan Wolking","doi":"10.1186/s42466-023-00248-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Discontinuing anti-seizure medication (ASM) should be considered in persons with epilepsy with long-term seizure freedom. Clinicians should also pursue ASM withdrawal in persons with one-time seizures without increased recurrence risk and those with suspected non-epileptic events. However, ASM withdrawal is associated with the risk of recurring seizures. Monitored ASM withdrawal in an epilepsy monitoring unit (EMU) could help better evaluate the risk of seizure recurrence. Here, we investigate the practice of EMU-guided ASM withdrawal, assess its indications, and aim to determine positive and negative predictors for successful withdrawal.</p><p><strong>Methods: </strong>We screened the medical records of all patients admitted to our EMU between November 1, 2019, and October 31, 2021, and included patients of at least 18 years admitted with the aim of permanent ASM withdrawal. We defined four groups of withdrawal indications: (1) long-term seizure freedom; (2) suspected non-epileptic events; (3) history of epileptic seizures but not fulfilling diagnostic criteria of epilepsy; and (4) seizure-freedom after epilepsy surgery. Successful withdrawal was defined according to the following criteria: no recoding of (sub)clinical seizure activity during VEM (groups 1, 2, and 3), patients did not meet the International League Against Epilepsy (ILAE) definition of epilepsy (groups 2 and 3) [14], and patients were discharged without ongoing ASM treatment (all groups). We also evaluated the prediction model by Lamberink et al. (LPM) for the risk of seizure recurrence in groups 1 and 3.</p><p><strong>Results: </strong>55/651 (8.6%) patients fulfilled the inclusion criteria. Withdrawal indications were distributed as follows; group 1: 2/55 (3.6%); group 2: 44/55 (80%); group 3: 9/55 (16,4%); group 4: 0/55. Overall, ASM withdrawal was successful in 90.9%. The sensitivity of the LPM for a 2-year 50% relapse risk threshold was 75%, the specificity 33.3%; for a 5-year relapse risk respectively 12.5% and 33.3%, suggesting that the model is not suitable for risk assessment in patients with one-time seizures or acute-symptomatic seizures, who constituted most of the evaluated patients.</p><p><strong>Conclusions: </strong>Our study suggests that EMU-guided ASM withdrawal could be a helpful tool to support clinical decision-making and improve patient safety. Prospective, randomized trials should further evaluate this method in the future.</p>","PeriodicalId":19169,"journal":{"name":"Neurological Research and Practice","volume":"5 1","pages":"20"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10193797/pdf/","citationCount":"1","resultStr":"{\"title\":\"Video-EEG-monitoring to guide antiseizure medication withdrawal.\",\"authors\":\"Laurien K L Dhaenens-Meyer, Elisabeth Schriewer, Yvonne G Weber, Stefan Wolking\",\"doi\":\"10.1186/s42466-023-00248-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Discontinuing anti-seizure medication (ASM) should be considered in persons with epilepsy with long-term seizure freedom. Clinicians should also pursue ASM withdrawal in persons with one-time seizures without increased recurrence risk and those with suspected non-epileptic events. However, ASM withdrawal is associated with the risk of recurring seizures. Monitored ASM withdrawal in an epilepsy monitoring unit (EMU) could help better evaluate the risk of seizure recurrence. Here, we investigate the practice of EMU-guided ASM withdrawal, assess its indications, and aim to determine positive and negative predictors for successful withdrawal.</p><p><strong>Methods: </strong>We screened the medical records of all patients admitted to our EMU between November 1, 2019, and October 31, 2021, and included patients of at least 18 years admitted with the aim of permanent ASM withdrawal. We defined four groups of withdrawal indications: (1) long-term seizure freedom; (2) suspected non-epileptic events; (3) history of epileptic seizures but not fulfilling diagnostic criteria of epilepsy; and (4) seizure-freedom after epilepsy surgery. Successful withdrawal was defined according to the following criteria: no recoding of (sub)clinical seizure activity during VEM (groups 1, 2, and 3), patients did not meet the International League Against Epilepsy (ILAE) definition of epilepsy (groups 2 and 3) [14], and patients were discharged without ongoing ASM treatment (all groups). We also evaluated the prediction model by Lamberink et al. (LPM) for the risk of seizure recurrence in groups 1 and 3.</p><p><strong>Results: </strong>55/651 (8.6%) patients fulfilled the inclusion criteria. Withdrawal indications were distributed as follows; group 1: 2/55 (3.6%); group 2: 44/55 (80%); group 3: 9/55 (16,4%); group 4: 0/55. Overall, ASM withdrawal was successful in 90.9%. The sensitivity of the LPM for a 2-year 50% relapse risk threshold was 75%, the specificity 33.3%; for a 5-year relapse risk respectively 12.5% and 33.3%, suggesting that the model is not suitable for risk assessment in patients with one-time seizures or acute-symptomatic seizures, who constituted most of the evaluated patients.</p><p><strong>Conclusions: </strong>Our study suggests that EMU-guided ASM withdrawal could be a helpful tool to support clinical decision-making and improve patient safety. Prospective, randomized trials should further evaluate this method in the future.</p>\",\"PeriodicalId\":19169,\"journal\":{\"name\":\"Neurological Research and Practice\",\"volume\":\"5 1\",\"pages\":\"20\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10193797/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurological Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42466-023-00248-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-023-00248-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Video-EEG-monitoring to guide antiseizure medication withdrawal.
Background: Discontinuing anti-seizure medication (ASM) should be considered in persons with epilepsy with long-term seizure freedom. Clinicians should also pursue ASM withdrawal in persons with one-time seizures without increased recurrence risk and those with suspected non-epileptic events. However, ASM withdrawal is associated with the risk of recurring seizures. Monitored ASM withdrawal in an epilepsy monitoring unit (EMU) could help better evaluate the risk of seizure recurrence. Here, we investigate the practice of EMU-guided ASM withdrawal, assess its indications, and aim to determine positive and negative predictors for successful withdrawal.
Methods: We screened the medical records of all patients admitted to our EMU between November 1, 2019, and October 31, 2021, and included patients of at least 18 years admitted with the aim of permanent ASM withdrawal. We defined four groups of withdrawal indications: (1) long-term seizure freedom; (2) suspected non-epileptic events; (3) history of epileptic seizures but not fulfilling diagnostic criteria of epilepsy; and (4) seizure-freedom after epilepsy surgery. Successful withdrawal was defined according to the following criteria: no recoding of (sub)clinical seizure activity during VEM (groups 1, 2, and 3), patients did not meet the International League Against Epilepsy (ILAE) definition of epilepsy (groups 2 and 3) [14], and patients were discharged without ongoing ASM treatment (all groups). We also evaluated the prediction model by Lamberink et al. (LPM) for the risk of seizure recurrence in groups 1 and 3.
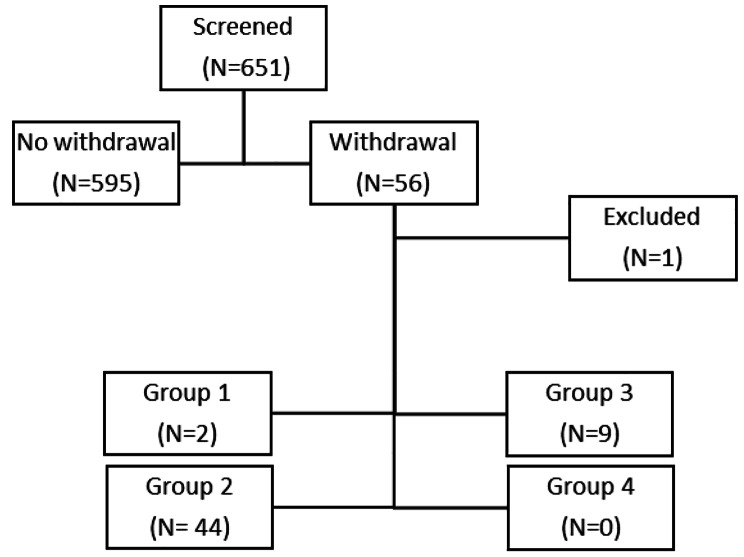
Results: 55/651 (8.6%) patients fulfilled the inclusion criteria. Withdrawal indications were distributed as follows; group 1: 2/55 (3.6%); group 2: 44/55 (80%); group 3: 9/55 (16,4%); group 4: 0/55. Overall, ASM withdrawal was successful in 90.9%. The sensitivity of the LPM for a 2-year 50% relapse risk threshold was 75%, the specificity 33.3%; for a 5-year relapse risk respectively 12.5% and 33.3%, suggesting that the model is not suitable for risk assessment in patients with one-time seizures or acute-symptomatic seizures, who constituted most of the evaluated patients.
Conclusions: Our study suggests that EMU-guided ASM withdrawal could be a helpful tool to support clinical decision-making and improve patient safety. Prospective, randomized trials should further evaluate this method in the future.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
