Venkatakrishna Rajajee, Reza Soroushmehr, Craig A Williamson, Kayvan Najarian, Kevin Ward, Hakam Tiba
{"title":"经颅彩色编码超声角度校正对颅内压升高的筛查作用。","authors":"Venkatakrishna Rajajee, Reza Soroushmehr, Craig A Williamson, Kayvan Najarian, Kevin Ward, Hakam Tiba","doi":"10.1097/CCE.0000000000000953","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Transcranial Doppler (TCD) has been evaluated as a noninvasive intracranial pressure (ICP) assessment tool. Correction for insonation angle, a potential source of error, with transcranial color-coded sonography (TCCS) has not previously been reported while evaluating ICP with TCD. Our objective was to study the accuracy of TCCS for detection of ICP elevation, with and without the use of angle correction.</p><p><strong>Design: </strong>Prospective study of diagnostic accuracy.</p><p><strong>Setting: </strong>Academic neurocritical care unit.</p><p><strong>Patients: </strong>Consecutive adults with invasive ICP monitors.</p><p><strong>Interventions: </strong>Ultrasound assessment with TCCS.</p><p><strong>Measurements and main results: </strong>End-diastolic velocity (EDV), time-averaged peak velocity (TAPV), and pulsatility index (PI) were measured in the bilateral middle cerebral arteries with and without angle correction. Concomitant mean arterial pressure (MAP) and ICP were recorded. Estimated cerebral perfusion pressure (CPP) was calculated as estimated CPP (CPPe) = MAP × (EDV/TAPV) + 14, and estimated ICP (ICPe) = MAP-CPPe. Sixty patients were enrolled and 55 underwent TCCS. Receiver operating characteristic curve analysis of ICPe for detection of invasive ICP greater than 22 mm Hg revealed area under the curve (AUC) 0.51 (0.37-0.64) without angle correction and 0.73 (0.58-0.84) with angle correction. The optimal threshold without angle correction was ICPe greater than 18 mm Hg with sensitivity 71% (29-96%) and specificity 28% (16-43%). With angle correction, the optimal threshold was ICPe greater than 21 mm Hg with sensitivity 100% (54-100%) and specificity 30% (17-46%). The AUC for PI was 0.61 (0.47-0.74) without angle correction and 0.70 (0.55-0.92) with angle correction.</p><p><strong>Conclusions: </strong>Angle correction improved the accuracy of TCCS for detection of elevated ICP. Sensitivity was high, as appropriate for a screening tool, but specificity remained low.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 9","pages":"e0953"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/ea/cc9-5-e0953.PMC10461938.pdf","citationCount":"1","resultStr":"{\"title\":\"Transcranial Color-Coded Sonography With Angle Correction As a Screening Tool for Raised Intracranial Pressure.\",\"authors\":\"Venkatakrishna Rajajee, Reza Soroushmehr, Craig A Williamson, Kayvan Najarian, Kevin Ward, Hakam Tiba\",\"doi\":\"10.1097/CCE.0000000000000953\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Transcranial Doppler (TCD) has been evaluated as a noninvasive intracranial pressure (ICP) assessment tool. Correction for insonation angle, a potential source of error, with transcranial color-coded sonography (TCCS) has not previously been reported while evaluating ICP with TCD. Our objective was to study the accuracy of TCCS for detection of ICP elevation, with and without the use of angle correction.</p><p><strong>Design: </strong>Prospective study of diagnostic accuracy.</p><p><strong>Setting: </strong>Academic neurocritical care unit.</p><p><strong>Patients: </strong>Consecutive adults with invasive ICP monitors.</p><p><strong>Interventions: </strong>Ultrasound assessment with TCCS.</p><p><strong>Measurements and main results: </strong>End-diastolic velocity (EDV), time-averaged peak velocity (TAPV), and pulsatility index (PI) were measured in the bilateral middle cerebral arteries with and without angle correction. Concomitant mean arterial pressure (MAP) and ICP were recorded. Estimated cerebral perfusion pressure (CPP) was calculated as estimated CPP (CPPe) = MAP × (EDV/TAPV) + 14, and estimated ICP (ICPe) = MAP-CPPe. Sixty patients were enrolled and 55 underwent TCCS. Receiver operating characteristic curve analysis of ICPe for detection of invasive ICP greater than 22 mm Hg revealed area under the curve (AUC) 0.51 (0.37-0.64) without angle correction and 0.73 (0.58-0.84) with angle correction. The optimal threshold without angle correction was ICPe greater than 18 mm Hg with sensitivity 71% (29-96%) and specificity 28% (16-43%). With angle correction, the optimal threshold was ICPe greater than 21 mm Hg with sensitivity 100% (54-100%) and specificity 30% (17-46%). The AUC for PI was 0.61 (0.47-0.74) without angle correction and 0.70 (0.55-0.92) with angle correction.</p><p><strong>Conclusions: </strong>Angle correction improved the accuracy of TCCS for detection of elevated ICP. Sensitivity was high, as appropriate for a screening tool, but specificity remained low.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 9\",\"pages\":\"e0953\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/ea/cc9-5-e0953.PMC10461938.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000953\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000953","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
目的:经颅多普勒(TCD)作为一种无创颅内压(ICP)评估工具。用经颅彩色编码超声(TCCS)校正超声角度,这是一个潜在的误差来源,以前没有报道过用TCD评估颅内压。我们的目的是研究TCCS检测ICP升高的准确性,无论是否使用角度校正。设计:诊断准确性的前瞻性研究。环境:学术神经危重症监护室。患者:连续使用有创ICP监护仪的成年人。干预措施:超声评估与TCCS。测量方法及主要结果:测量双侧大脑中动脉舒张末期速度(EDV)、时间平均峰值速度(TAPV)和脉搏指数(PI)。同时记录平均动脉压(MAP)和颅内压(ICP)。估算脑灌注压(CPP)计算为估算CPP (CPPe) = MAP × (EDV/TAPV) + 14,估算ICP (ICPe) = MAP-CPPe。60例患者入组,55例接受TCCS。ICPe检测大于22 mm Hg有侵入性ICP的受试者工作特征曲线分析显示,无角度校正的曲线下面积(AUC)为0.51(0.37 ~ 0.64),有角度校正的AUC为0.73(0.58 ~ 0.84)。无角度校正的最佳阈值为ICPe大于18 mm Hg,敏感性71%(29-96%),特异性28%(16-43%)。角度校正后,最佳阈值为ICPe大于21 mm Hg,灵敏度100%(54-100%),特异性30%(17-46%)。无角度校正的PI AUC为0.61(0.47 ~ 0.74),有角度校正的PI AUC为0.70(0.55 ~ 0.92)。结论:角度校正提高了TCCS检测颅内压升高的准确性。灵敏度高,作为合适的筛选工具,但特异性仍然很低。
Transcranial Color-Coded Sonography With Angle Correction As a Screening Tool for Raised Intracranial Pressure.
Objectives: Transcranial Doppler (TCD) has been evaluated as a noninvasive intracranial pressure (ICP) assessment tool. Correction for insonation angle, a potential source of error, with transcranial color-coded sonography (TCCS) has not previously been reported while evaluating ICP with TCD. Our objective was to study the accuracy of TCCS for detection of ICP elevation, with and without the use of angle correction.
Design: Prospective study of diagnostic accuracy.
Setting: Academic neurocritical care unit.
Patients: Consecutive adults with invasive ICP monitors.
Interventions: Ultrasound assessment with TCCS.
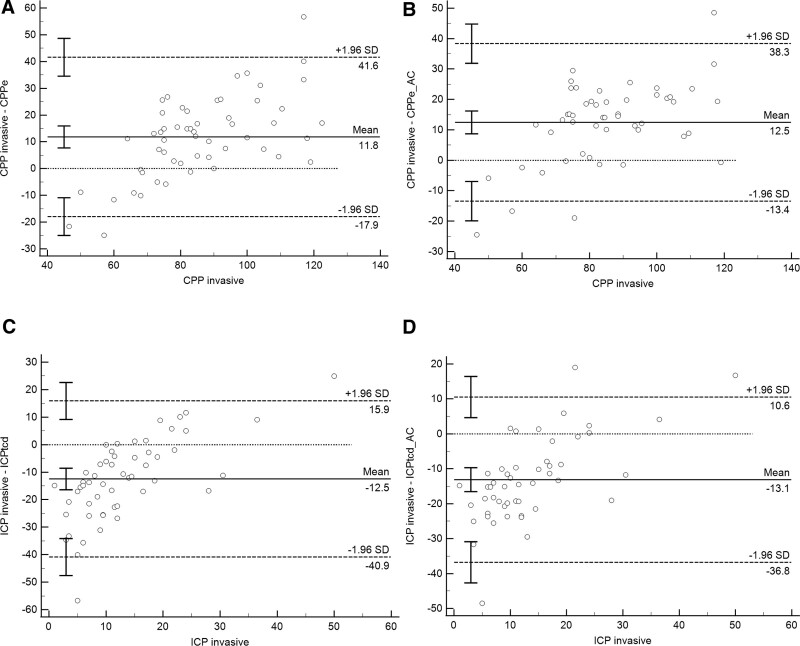
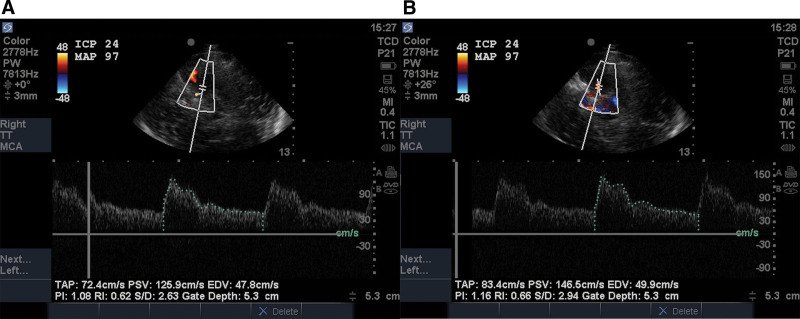
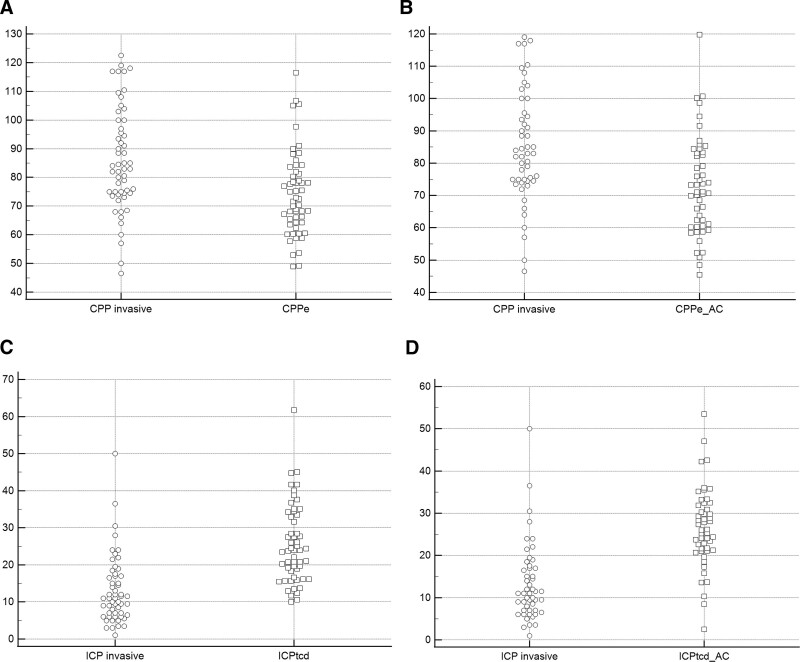
Measurements and main results: End-diastolic velocity (EDV), time-averaged peak velocity (TAPV), and pulsatility index (PI) were measured in the bilateral middle cerebral arteries with and without angle correction. Concomitant mean arterial pressure (MAP) and ICP were recorded. Estimated cerebral perfusion pressure (CPP) was calculated as estimated CPP (CPPe) = MAP × (EDV/TAPV) + 14, and estimated ICP (ICPe) = MAP-CPPe. Sixty patients were enrolled and 55 underwent TCCS. Receiver operating characteristic curve analysis of ICPe for detection of invasive ICP greater than 22 mm Hg revealed area under the curve (AUC) 0.51 (0.37-0.64) without angle correction and 0.73 (0.58-0.84) with angle correction. The optimal threshold without angle correction was ICPe greater than 18 mm Hg with sensitivity 71% (29-96%) and specificity 28% (16-43%). With angle correction, the optimal threshold was ICPe greater than 21 mm Hg with sensitivity 100% (54-100%) and specificity 30% (17-46%). The AUC for PI was 0.61 (0.47-0.74) without angle correction and 0.70 (0.55-0.92) with angle correction.
Conclusions: Angle correction improved the accuracy of TCCS for detection of elevated ICP. Sensitivity was high, as appropriate for a screening tool, but specificity remained low.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
