Gil Joon Suh, Tae Gun Shin, Woon Yong Kwon, Kyuseok Kim, You Hwan Jo, Sung-Hyuk Choi, Sung Phil Chung, Won Young Kim
{"title":"脓毒症休克的血液动力学管理:超越脓毒症生存运动指南。","authors":"Gil Joon Suh, Tae Gun Shin, Woon Yong Kwon, Kyuseok Kim, You Hwan Jo, Sung-Hyuk Choi, Sung Phil Chung, Won Young Kim","doi":"10.15441/ceem.23.065","DOIUrl":null,"url":null,"abstract":"<p><p>Although the Surviving Sepsis Campaign guidelines provide standardized and generalized guidance, they are less individualized. This review focuses on recent updates in the hemodynamic management of septic shock. Monitoring and intervention for septic shock should be personalized according to the phase of shock. In the salvage phase, fluid resuscitation and vasopressors should be given to provide life-saving tissue perfusion. During the optimization phase, tissue perfusion should be optimized. In the stabilization and de-escalation phases, minimal fluid infusion and safe fluid removal should be performed, respectively, while preserving organ perfusion. There is controversy surrounding the use of restrictive versus liberal fluid strategies after initial resuscitation. Fluid administration after initial resuscitation should depend upon the patient's fluid responsiveness and requires individualized management. A number of dynamic tests have been proposed to monitor fluid responsiveness, which can help clinicians decide whether to give fluid or not. The optimal timing for the initiation of vasopressor agents is unknown. Recent data suggest that early vasopressor initiation should be considered. Inotropes can be considered in patients with decreased cardiac contractility associated with impaired tissue perfusion despite adequate volume status and arterial blood pressure. Venoarterial extracorporeal membrane oxygenation should be considered for refractory septic shock with severe cardiac systolic dysfunction.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"255-264"},"PeriodicalIF":2.3000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/23/5b/ceem-23-065.PMC10579730.pdf","citationCount":"0","resultStr":"{\"title\":\"Hemodynamic management of septic shock: beyond the Surviving Sepsis Campaign guidelines.\",\"authors\":\"Gil Joon Suh, Tae Gun Shin, Woon Yong Kwon, Kyuseok Kim, You Hwan Jo, Sung-Hyuk Choi, Sung Phil Chung, Won Young Kim\",\"doi\":\"10.15441/ceem.23.065\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Although the Surviving Sepsis Campaign guidelines provide standardized and generalized guidance, they are less individualized. This review focuses on recent updates in the hemodynamic management of septic shock. Monitoring and intervention for septic shock should be personalized according to the phase of shock. In the salvage phase, fluid resuscitation and vasopressors should be given to provide life-saving tissue perfusion. During the optimization phase, tissue perfusion should be optimized. In the stabilization and de-escalation phases, minimal fluid infusion and safe fluid removal should be performed, respectively, while preserving organ perfusion. There is controversy surrounding the use of restrictive versus liberal fluid strategies after initial resuscitation. Fluid administration after initial resuscitation should depend upon the patient's fluid responsiveness and requires individualized management. A number of dynamic tests have been proposed to monitor fluid responsiveness, which can help clinicians decide whether to give fluid or not. The optimal timing for the initiation of vasopressor agents is unknown. Recent data suggest that early vasopressor initiation should be considered. Inotropes can be considered in patients with decreased cardiac contractility associated with impaired tissue perfusion despite adequate volume status and arterial blood pressure. Venoarterial extracorporeal membrane oxygenation should be considered for refractory septic shock with severe cardiac systolic dysfunction.</p>\",\"PeriodicalId\":10325,\"journal\":{\"name\":\"Clinical and Experimental Emergency Medicine\",\"volume\":\" \",\"pages\":\"255-264\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/23/5b/ceem-23-065.PMC10579730.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15441/ceem.23.065\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.23.065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Hemodynamic management of septic shock: beyond the Surviving Sepsis Campaign guidelines.
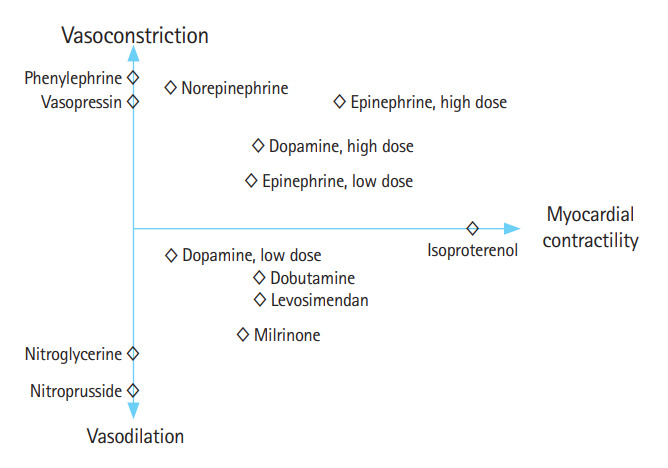
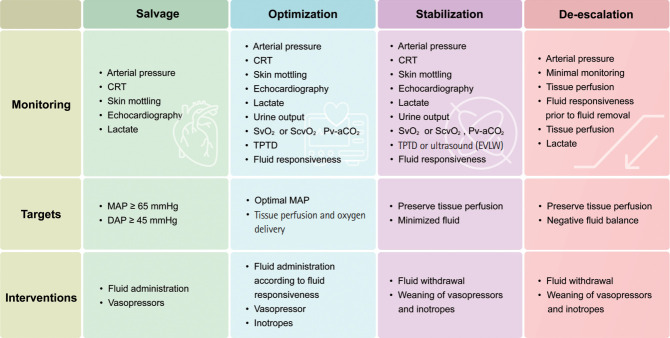
Although the Surviving Sepsis Campaign guidelines provide standardized and generalized guidance, they are less individualized. This review focuses on recent updates in the hemodynamic management of septic shock. Monitoring and intervention for septic shock should be personalized according to the phase of shock. In the salvage phase, fluid resuscitation and vasopressors should be given to provide life-saving tissue perfusion. During the optimization phase, tissue perfusion should be optimized. In the stabilization and de-escalation phases, minimal fluid infusion and safe fluid removal should be performed, respectively, while preserving organ perfusion. There is controversy surrounding the use of restrictive versus liberal fluid strategies after initial resuscitation. Fluid administration after initial resuscitation should depend upon the patient's fluid responsiveness and requires individualized management. A number of dynamic tests have been proposed to monitor fluid responsiveness, which can help clinicians decide whether to give fluid or not. The optimal timing for the initiation of vasopressor agents is unknown. Recent data suggest that early vasopressor initiation should be considered. Inotropes can be considered in patients with decreased cardiac contractility associated with impaired tissue perfusion despite adequate volume status and arterial blood pressure. Venoarterial extracorporeal membrane oxygenation should be considered for refractory septic shock with severe cardiac systolic dysfunction.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
