{"title":"罕见的由阿伯内蒂畸形(IIC型)引起的门静脉高压1例。","authors":"Xin Yao, Yang Liu, Li-Dan Yu, Jian-Ping Qin","doi":"10.4329/wjr.v15.i8.250","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abernethy malformation is a rare congenital vascular malformation with a portosystemic shunt that may clinically manifest as cholestasis, dyspnea, or hepatic encephalopathy, among other conditions. Early diagnosis and classification are very important to further guide treatment. Typically, patients with congenital portosystemic shunts have no characteristics of portal hypertension. Herein, we report an 18-year-old female with prominent portal hypertension that manifested mainly as rupture and bleeding of esophageal varices. Imaging showed a thin main portal vein, no portal vein branches in the liver, and bleeding of the esophageal and gastric varices caused by the collateral circulation upwards from the proximal main portal vein. Patients with Abernethy malformation type I are usually treated with liver transplantation, and patients with type II are treated with shunt occlusion, surgery, or transcatheter coiling. Our patient was treated with endoscopic surgery combined with drug therapy and had no portal hypertension and good hepatic function for 24 mo of follow-up.</p><p><strong>Case summary: </strong>This case report describes our experience in the diagnosis and treatment of an 18-year-old female with Abernethy malformation type IIC and portal hypertension. This condition was initially diagnosed as cirrhosis combined with portal hypertension. The patient was ultimately diagnosed using liver histology and subsequent imaging, and the treatment was highly effective. To publish this case report, written informed consent was obtained from the patient, including the attached imaging data.</p><p><strong>Conclusion: </strong>Abernethy malformation type IIC may develop portal hypertension, and traditional nonselective beta-blockers combined with endoscopic treatment can achieve high efficacy.</p>","PeriodicalId":23819,"journal":{"name":"World journal of radiology","volume":"15 8","pages":"250-255"},"PeriodicalIF":1.5000,"publicationDate":"2023-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/51/WJR-15-250.PMC10473916.pdf","citationCount":"0","resultStr":"{\"title\":\"Rare portal hypertension caused by Abernethy malformation (Type IIC): A case report.\",\"authors\":\"Xin Yao, Yang Liu, Li-Dan Yu, Jian-Ping Qin\",\"doi\":\"10.4329/wjr.v15.i8.250\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Abernethy malformation is a rare congenital vascular malformation with a portosystemic shunt that may clinically manifest as cholestasis, dyspnea, or hepatic encephalopathy, among other conditions. Early diagnosis and classification are very important to further guide treatment. Typically, patients with congenital portosystemic shunts have no characteristics of portal hypertension. Herein, we report an 18-year-old female with prominent portal hypertension that manifested mainly as rupture and bleeding of esophageal varices. Imaging showed a thin main portal vein, no portal vein branches in the liver, and bleeding of the esophageal and gastric varices caused by the collateral circulation upwards from the proximal main portal vein. Patients with Abernethy malformation type I are usually treated with liver transplantation, and patients with type II are treated with shunt occlusion, surgery, or transcatheter coiling. Our patient was treated with endoscopic surgery combined with drug therapy and had no portal hypertension and good hepatic function for 24 mo of follow-up.</p><p><strong>Case summary: </strong>This case report describes our experience in the diagnosis and treatment of an 18-year-old female with Abernethy malformation type IIC and portal hypertension. This condition was initially diagnosed as cirrhosis combined with portal hypertension. The patient was ultimately diagnosed using liver histology and subsequent imaging, and the treatment was highly effective. To publish this case report, written informed consent was obtained from the patient, including the attached imaging data.</p><p><strong>Conclusion: </strong>Abernethy malformation type IIC may develop portal hypertension, and traditional nonselective beta-blockers combined with endoscopic treatment can achieve high efficacy.</p>\",\"PeriodicalId\":23819,\"journal\":{\"name\":\"World journal of radiology\",\"volume\":\"15 8\",\"pages\":\"250-255\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/51/WJR-15-250.PMC10473916.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4329/wjr.v15.i8.250\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4329/wjr.v15.i8.250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Rare portal hypertension caused by Abernethy malformation (Type IIC): A case report.
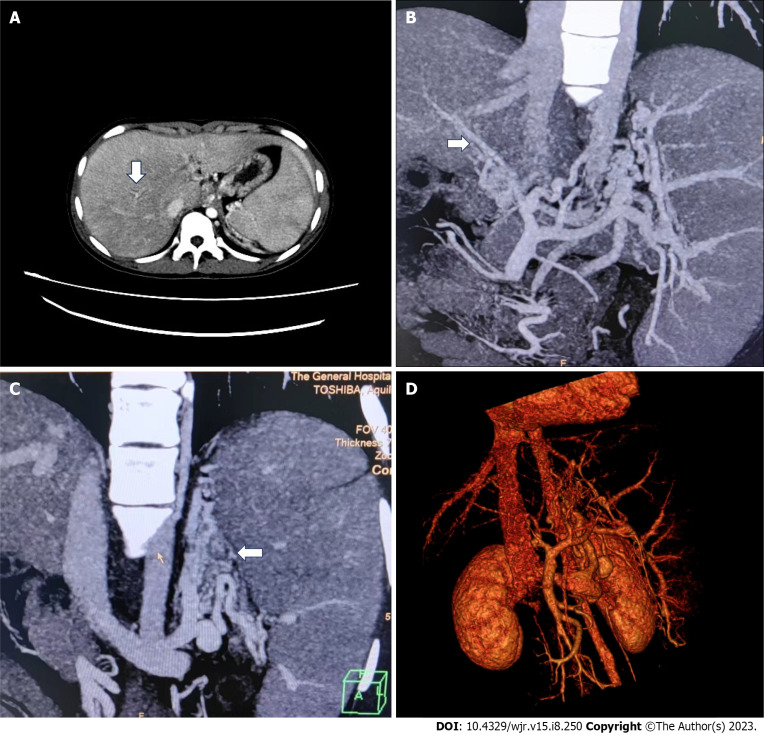
Background: Abernethy malformation is a rare congenital vascular malformation with a portosystemic shunt that may clinically manifest as cholestasis, dyspnea, or hepatic encephalopathy, among other conditions. Early diagnosis and classification are very important to further guide treatment. Typically, patients with congenital portosystemic shunts have no characteristics of portal hypertension. Herein, we report an 18-year-old female with prominent portal hypertension that manifested mainly as rupture and bleeding of esophageal varices. Imaging showed a thin main portal vein, no portal vein branches in the liver, and bleeding of the esophageal and gastric varices caused by the collateral circulation upwards from the proximal main portal vein. Patients with Abernethy malformation type I are usually treated with liver transplantation, and patients with type II are treated with shunt occlusion, surgery, or transcatheter coiling. Our patient was treated with endoscopic surgery combined with drug therapy and had no portal hypertension and good hepatic function for 24 mo of follow-up.
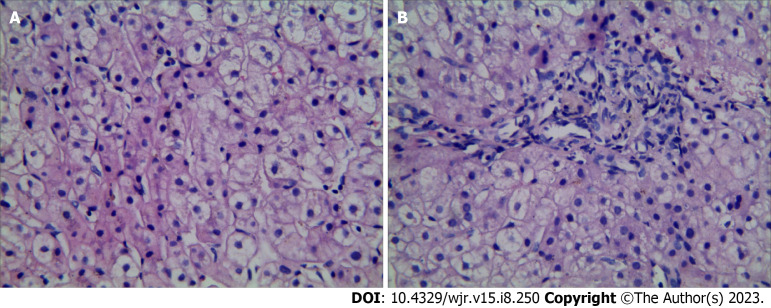
Case summary: This case report describes our experience in the diagnosis and treatment of an 18-year-old female with Abernethy malformation type IIC and portal hypertension. This condition was initially diagnosed as cirrhosis combined with portal hypertension. The patient was ultimately diagnosed using liver histology and subsequent imaging, and the treatment was highly effective. To publish this case report, written informed consent was obtained from the patient, including the attached imaging data.
Conclusion: Abernethy malformation type IIC may develop portal hypertension, and traditional nonselective beta-blockers combined with endoscopic treatment can achieve high efficacy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
