Joshua Weiner, Nathaly Llore, Dylan Ormsby, Masato Fujiki, Maria Cristina Segovia, Mark Obri, Syed-Mohammed Jafri, Jedson Liggett, Alexander H K Kroemer, Cal Matsumoto, Jang Moon, Pierpaolo Di Cocco, Gennaro Selvaggi, Jennifer Garcia, Armando Ganoza, Ajai Khanna, George Mazariegos, Danielle Wendel, Jorge Reyes
{"title":"美国肠道移植中心免疫抑制实践的首次集体检查。","authors":"Joshua Weiner, Nathaly Llore, Dylan Ormsby, Masato Fujiki, Maria Cristina Segovia, Mark Obri, Syed-Mohammed Jafri, Jedson Liggett, Alexander H K Kroemer, Cal Matsumoto, Jang Moon, Pierpaolo Di Cocco, Gennaro Selvaggi, Jennifer Garcia, Armando Ganoza, Ajai Khanna, George Mazariegos, Danielle Wendel, Jorge Reyes","doi":"10.1097/TXD.0000000000001512","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unlike other solid organs, no standardized treatment algorithms exist for intestinal transplantation (ITx). We established a consortium of American ITx centers to evaluate current practices.</p><p><strong>Methods: </strong>All American centers performing ITx during the past 3 y were invited to participate. As a consortium, we generated questions to evaluate and collect data from each institution. The data were compiled and analyzed.</p><p><strong>Results: </strong>Ten centers participated, performing 211 ITx during the past 3 y (range, 3-46; mean 21.1). Induction regimens varied widely. Thymoglobulin was the most common, used in the plurality of patients (85/211; 40.3%), but there was no consensus regimen. Similarly, regimens for the treatment of acute cellular rejection, antibody-mediated rejection, and graft-versus-host disease varied significantly between centers. We also evaluated differences in maintenance immunosuppression protocols, desensitization regimens, mammalian target of rapamycin use, antimetabolite use, and posttransplantation surveillance practices. Maintenance tacrolimus levels, stoma presence, and scoping frequency were not associated with differences in rejection events. Definitive association between treatments and outcomes, including graft and patient survival, was not the intention of this initial collaboration and is prevented by the lack of patient-level data and the presence of confounders. However, we identified trends regarding rejection episodes after various induction strategies that require further investigation in our subsequent collaborations.</p><p><strong>Conclusions: </strong>This initial collaboration reveals the extreme heterogeneity of practices among American ITx centers. Future collaboration will explore patient-level data, stratified by age and transplant type (isolated intestine versus multivisceral), to explore the association between treatment regimens and outcomes.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"9 9","pages":"e1512"},"PeriodicalIF":2.2000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/ca/txd-9-e1512.PMC10455426.pdf","citationCount":"0","resultStr":"{\"title\":\"The First Collective Examination of Immunosuppressive Practices Among American Intestinal Transplant Centers.\",\"authors\":\"Joshua Weiner, Nathaly Llore, Dylan Ormsby, Masato Fujiki, Maria Cristina Segovia, Mark Obri, Syed-Mohammed Jafri, Jedson Liggett, Alexander H K Kroemer, Cal Matsumoto, Jang Moon, Pierpaolo Di Cocco, Gennaro Selvaggi, Jennifer Garcia, Armando Ganoza, Ajai Khanna, George Mazariegos, Danielle Wendel, Jorge Reyes\",\"doi\":\"10.1097/TXD.0000000000001512\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Unlike other solid organs, no standardized treatment algorithms exist for intestinal transplantation (ITx). We established a consortium of American ITx centers to evaluate current practices.</p><p><strong>Methods: </strong>All American centers performing ITx during the past 3 y were invited to participate. As a consortium, we generated questions to evaluate and collect data from each institution. The data were compiled and analyzed.</p><p><strong>Results: </strong>Ten centers participated, performing 211 ITx during the past 3 y (range, 3-46; mean 21.1). Induction regimens varied widely. Thymoglobulin was the most common, used in the plurality of patients (85/211; 40.3%), but there was no consensus regimen. Similarly, regimens for the treatment of acute cellular rejection, antibody-mediated rejection, and graft-versus-host disease varied significantly between centers. We also evaluated differences in maintenance immunosuppression protocols, desensitization regimens, mammalian target of rapamycin use, antimetabolite use, and posttransplantation surveillance practices. Maintenance tacrolimus levels, stoma presence, and scoping frequency were not associated with differences in rejection events. Definitive association between treatments and outcomes, including graft and patient survival, was not the intention of this initial collaboration and is prevented by the lack of patient-level data and the presence of confounders. However, we identified trends regarding rejection episodes after various induction strategies that require further investigation in our subsequent collaborations.</p><p><strong>Conclusions: </strong>This initial collaboration reveals the extreme heterogeneity of practices among American ITx centers. Future collaboration will explore patient-level data, stratified by age and transplant type (isolated intestine versus multivisceral), to explore the association between treatment regimens and outcomes.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"9 9\",\"pages\":\"e1512\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/ca/txd-9-e1512.PMC10455426.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001512\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001512","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
The First Collective Examination of Immunosuppressive Practices Among American Intestinal Transplant Centers.
Background: Unlike other solid organs, no standardized treatment algorithms exist for intestinal transplantation (ITx). We established a consortium of American ITx centers to evaluate current practices.
Methods: All American centers performing ITx during the past 3 y were invited to participate. As a consortium, we generated questions to evaluate and collect data from each institution. The data were compiled and analyzed.
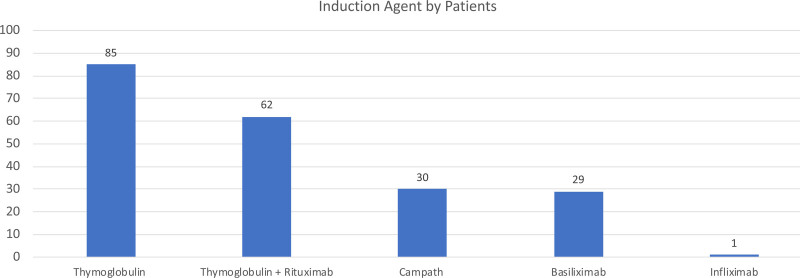
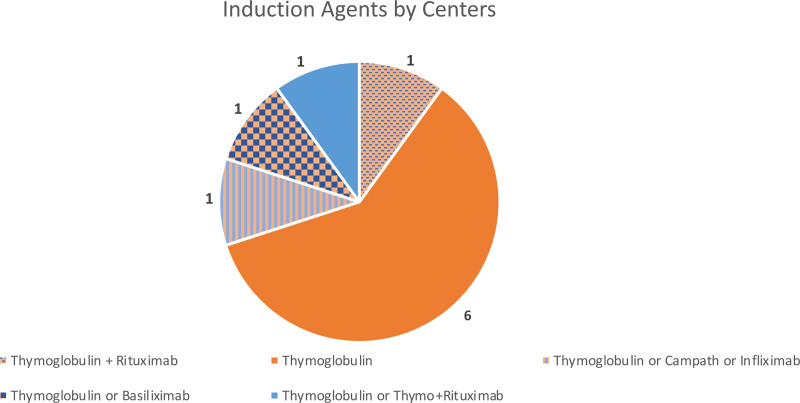
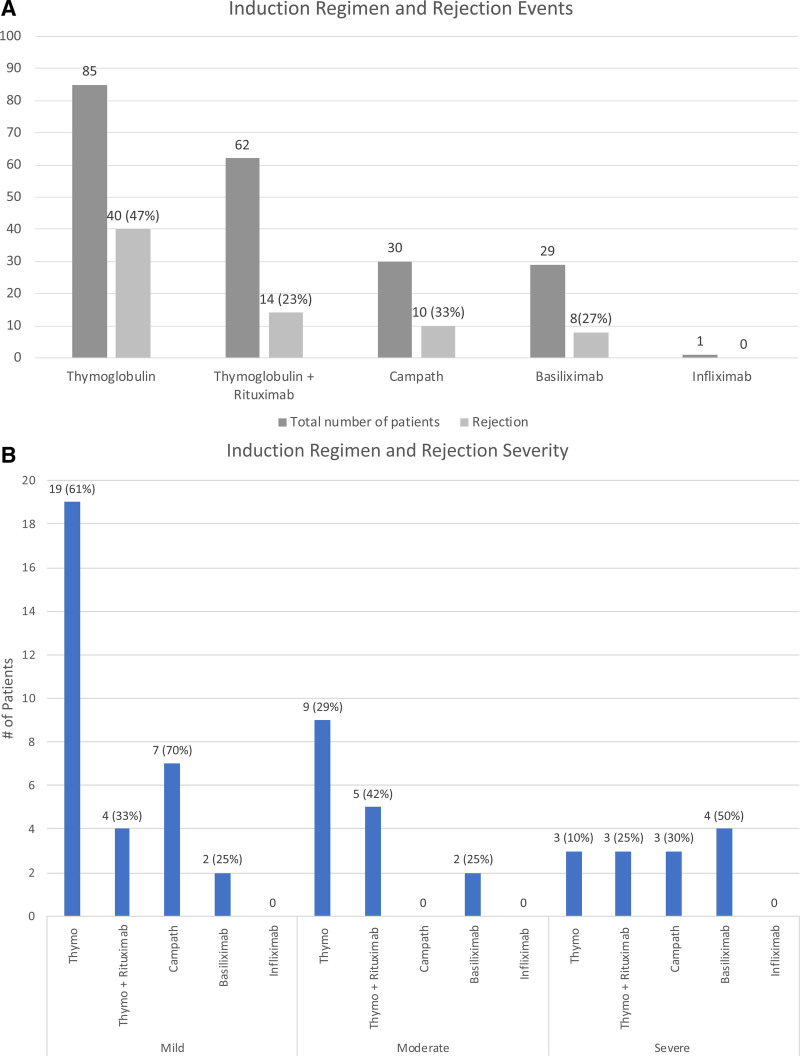
Results: Ten centers participated, performing 211 ITx during the past 3 y (range, 3-46; mean 21.1). Induction regimens varied widely. Thymoglobulin was the most common, used in the plurality of patients (85/211; 40.3%), but there was no consensus regimen. Similarly, regimens for the treatment of acute cellular rejection, antibody-mediated rejection, and graft-versus-host disease varied significantly between centers. We also evaluated differences in maintenance immunosuppression protocols, desensitization regimens, mammalian target of rapamycin use, antimetabolite use, and posttransplantation surveillance practices. Maintenance tacrolimus levels, stoma presence, and scoping frequency were not associated with differences in rejection events. Definitive association between treatments and outcomes, including graft and patient survival, was not the intention of this initial collaboration and is prevented by the lack of patient-level data and the presence of confounders. However, we identified trends regarding rejection episodes after various induction strategies that require further investigation in our subsequent collaborations.
Conclusions: This initial collaboration reveals the extreme heterogeneity of practices among American ITx centers. Future collaboration will explore patient-level data, stratified by age and transplant type (isolated intestine versus multivisceral), to explore the association between treatment regimens and outcomes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
