Michihiro Suwa, Yuki Nohara, Isao Morii, Masaya Kino
{"title":"在非瓣膜性房颤患者血浆浓度监测中对依多沙班和利伐沙班剂量的安全性和有效性进行再评价:标签上和标签外剂量的观察","authors":"Michihiro Suwa, Yuki Nohara, Isao Morii, Masaya Kino","doi":"10.1253/circrep.CR-22-0076","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Background:</i></b> Off-label dosing of direct oral anticoagulants (DOAC) as a treatment for non-valvular atrial fibrillation (NVAF) is problematic. Here, we investigated the status of rivaroxaban and edoxaban dosing by monitoring plasma concentrations (PCs). <b><i>Methods and Results:</i></b> We monitored drug PCs in 391 and 333 outpatients receiving rivaroxaban and edoxaban, respectively, for NVAF. Drug doses were adjusted if the PC was above the cut-off value (rivaroxaban: 404 ng/mL; edoxaban: 402 ng/mL), determined from receiver operating characteristic curves for predicting bleeding events. On-label standard dosing was reduced to off-label underdosing due to high PCs above the cut-off more often for rivaroxaban (28.1%) than edoxaban (12.6%; P<0.001). Over a median follow-up of 13 months for rivaroxaban and 10 months for edoxaban, the annual incidence of bleeding events was higher with rivaroxaban than with edoxaban (4.88 vs. 3.73 patient-years; P<0.05), although no thromboembolic events occurred in either group. Furthermore, for patients with creatinine clearance >50 mL/min and body weight ≤60 kg, there was a greater incidence of bleeding events with rivaroxaban on-label 15 mg dosing than with edoxaban on-label 30 mg dosing (22.2% vs 2.9%; P<0.01). <b><i>Conclusions:</i></b> Monitoring the PCs of rivaroxaban and edoxaban in NVAF patients enables dose adjustments to reduce bleeding risk. The incidence of bleeding under drug PC monitoring was less in the edoxaban than rivaroxaban group.</p>","PeriodicalId":10276,"journal":{"name":"Circulation Reports","volume":"5 3","pages":"80-89"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/e2/circrep-5-80.PMC9992501.pdf","citationCount":"0","resultStr":"{\"title\":\"Safety and Efficacy Re-Evaluation of Edoxaban and Rivaroxaban Dosing With Plasma Concentration Monitoring in Non-Valvular Atrial Fibrillation: With Observations of On-Label and Off-Label Dosing.\",\"authors\":\"Michihiro Suwa, Yuki Nohara, Isao Morii, Masaya Kino\",\"doi\":\"10.1253/circrep.CR-22-0076\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b><i>Background:</i></b> Off-label dosing of direct oral anticoagulants (DOAC) as a treatment for non-valvular atrial fibrillation (NVAF) is problematic. Here, we investigated the status of rivaroxaban and edoxaban dosing by monitoring plasma concentrations (PCs). <b><i>Methods and Results:</i></b> We monitored drug PCs in 391 and 333 outpatients receiving rivaroxaban and edoxaban, respectively, for NVAF. Drug doses were adjusted if the PC was above the cut-off value (rivaroxaban: 404 ng/mL; edoxaban: 402 ng/mL), determined from receiver operating characteristic curves for predicting bleeding events. On-label standard dosing was reduced to off-label underdosing due to high PCs above the cut-off more often for rivaroxaban (28.1%) than edoxaban (12.6%; P<0.001). Over a median follow-up of 13 months for rivaroxaban and 10 months for edoxaban, the annual incidence of bleeding events was higher with rivaroxaban than with edoxaban (4.88 vs. 3.73 patient-years; P<0.05), although no thromboembolic events occurred in either group. Furthermore, for patients with creatinine clearance >50 mL/min and body weight ≤60 kg, there was a greater incidence of bleeding events with rivaroxaban on-label 15 mg dosing than with edoxaban on-label 30 mg dosing (22.2% vs 2.9%; P<0.01). <b><i>Conclusions:</i></b> Monitoring the PCs of rivaroxaban and edoxaban in NVAF patients enables dose adjustments to reduce bleeding risk. The incidence of bleeding under drug PC monitoring was less in the edoxaban than rivaroxaban group.</p>\",\"PeriodicalId\":10276,\"journal\":{\"name\":\"Circulation Reports\",\"volume\":\"5 3\",\"pages\":\"80-89\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/e2/circrep-5-80.PMC9992501.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1253/circrep.CR-22-0076\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-22-0076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
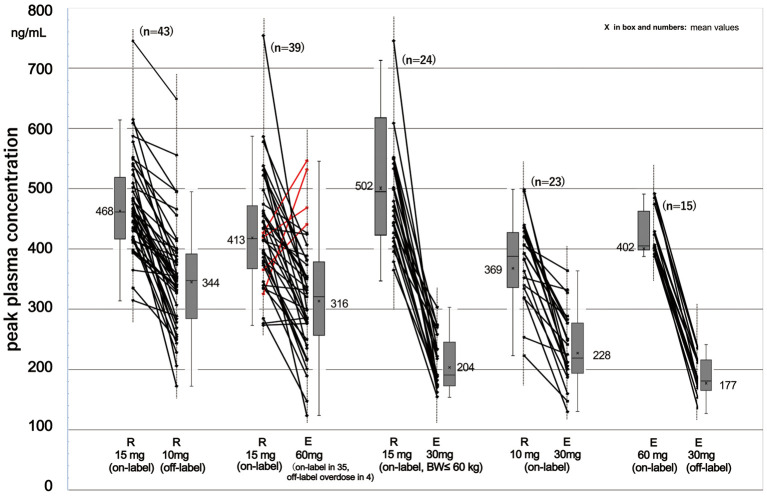
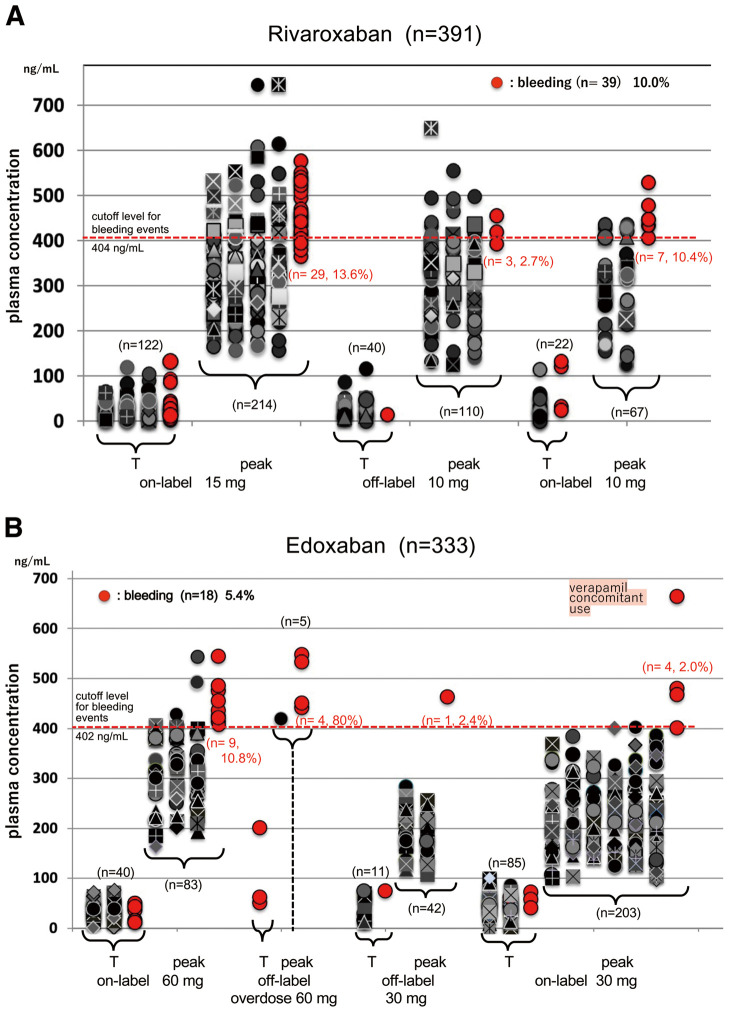
背景:直接口服抗凝剂(DOAC)作为非瓣膜性房颤(NVAF)治疗的超说明书剂量是有问题的。在这里,我们通过监测血浆浓度(PCs)来研究利伐沙班和依多沙班的剂量状况。方法与结果:我们分别对391例和333例接受利伐沙班和依多沙班治疗非瓣膜性房颤的门诊患者进行药物PCs监测。如果PC高于临界值(利伐沙班:404 ng/mL;依多沙班:402 ng/mL),根据受试者工作特征曲线测定,用于预测出血事件。由于利伐沙班(28.1%)比依多沙班(12.6%)的pc值高于临界值,标签上的标准剂量减少到标签外的不足剂量;P50 mL/min,体重≤60 kg时,利伐沙班标签上15mg剂量组出血事件发生率高于标签上30mg剂量组(22.2% vs 2.9%;结论:监测非瓣膜性房颤患者利伐沙班和依多沙班的PCs可调整剂量以降低出血风险。药物PC监测下,依多沙班组出血发生率低于利伐沙班组。
Safety and Efficacy Re-Evaluation of Edoxaban and Rivaroxaban Dosing With Plasma Concentration Monitoring in Non-Valvular Atrial Fibrillation: With Observations of On-Label and Off-Label Dosing.
Background: Off-label dosing of direct oral anticoagulants (DOAC) as a treatment for non-valvular atrial fibrillation (NVAF) is problematic. Here, we investigated the status of rivaroxaban and edoxaban dosing by monitoring plasma concentrations (PCs). Methods and Results: We monitored drug PCs in 391 and 333 outpatients receiving rivaroxaban and edoxaban, respectively, for NVAF. Drug doses were adjusted if the PC was above the cut-off value (rivaroxaban: 404 ng/mL; edoxaban: 402 ng/mL), determined from receiver operating characteristic curves for predicting bleeding events. On-label standard dosing was reduced to off-label underdosing due to high PCs above the cut-off more often for rivaroxaban (28.1%) than edoxaban (12.6%; P<0.001). Over a median follow-up of 13 months for rivaroxaban and 10 months for edoxaban, the annual incidence of bleeding events was higher with rivaroxaban than with edoxaban (4.88 vs. 3.73 patient-years; P<0.05), although no thromboembolic events occurred in either group. Furthermore, for patients with creatinine clearance >50 mL/min and body weight ≤60 kg, there was a greater incidence of bleeding events with rivaroxaban on-label 15 mg dosing than with edoxaban on-label 30 mg dosing (22.2% vs 2.9%; P<0.01). Conclusions: Monitoring the PCs of rivaroxaban and edoxaban in NVAF patients enables dose adjustments to reduce bleeding risk. The incidence of bleeding under drug PC monitoring was less in the edoxaban than rivaroxaban group.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
