Amy Eckland, Michael Kohut, Henry Stoddard, Deb Burris, Frank Chessa, Monica K Sikka, Daniel A Solomon, Colleen M Kershaw, Ellen F Eaton, Rebecca Hutchinson, Peter D Friedmann, Thomas J Stopka, Kathleen M Fairfield, Kinna Thakarar
{"title":"“我比任何人都更了解我的身体”:一项关于有实际经验的人对注射药物使用相关感染的抗菌治疗决策的观点的定性研究。","authors":"Amy Eckland, Michael Kohut, Henry Stoddard, Deb Burris, Frank Chessa, Monica K Sikka, Daniel A Solomon, Colleen M Kershaw, Ellen F Eaton, Rebecca Hutchinson, Peter D Friedmann, Thomas J Stopka, Kathleen M Fairfield, Kinna Thakarar","doi":"10.1177/20499361231197065","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>People who inject drugs (PWID) are at risk for severe bacterial and fungal infections including skin and soft tissue infections, endocarditis, and osteomyelitis. PWID have high rates of self-directed discharge and are often not offered outpatient antimicrobial therapies, despite studies showing their efficacy and safety in PWID. This study fills a gap in knowledge of patient and community partner perspectives on treatment and discharge decision making for injection drug use (IDU)-associated infections.</p><p><strong>Methods: </strong>We conducted semi-structured interviews with patients (<i>n</i> = 10) hospitalized with IDU-associated infections and community partners (<i>n</i> = 6) in the Portland, Maine region. Community partners include peer support workers at syringe services programs (SSPs) and outreach specialists working with PWID. We transcribed and thematically analyzed interviews to explore perspectives on three domains: perspectives on long-term hospitalization, outpatient treatment options, and patient involvement in decision making.</p><p><strong>Results: </strong>Participants noted that stigma and inadequate pain management created poor hospitalization experiences that contributed to self-directed discharge. On the other hand, patients reported hospitalization provided opportunities to connect to substance use disorder (SUD) treatment and protect them from outside substance use triggers. Many patients expressed interest in outpatient antimicrobial treatment options conditional upon perceived efficacy of the treatment, perceived ability to complete treatment, and available resources and social support. Finally, both patients and community partners emphasized the importance of autonomy and inclusion in medical decision making. Although some participants acknowledged their SUD, withdrawal symptoms, or undertreated pain might interfere with decision making, they felt these medical conditions were not justification for health care professionals withholding treatment options. They recommended open communication to build trust and reduce harms.</p><p><strong>Conclusion: </strong>Patients with IDU-associated infections desire autonomy, respect, and patient-centered care from healthcare workers, and may self-discharge when needs or preferences are not met. Involving patients in treatment decisions and offering outpatient antimicrobial options may result in better outcomes. However, patient involvement in decision making may be complicated by many contextual factors unique to each patient, suggesting a need for shared decision making to meet the needs of hospitalized patients with IDU-associated infections.</p>","PeriodicalId":46154,"journal":{"name":"Therapeutic Advances in Infectious Disease","volume":"10 ","pages":"20499361231197065"},"PeriodicalIF":3.4000,"publicationDate":"2023-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/f6/10.1177_20499361231197065.PMC10492466.pdf","citationCount":"0","resultStr":"{\"title\":\"\\\"I know my body better than anyone else\\\": a qualitative study of perspectives of people with lived experience on antimicrobial treatment decisions for injection drug use-associated infections.\",\"authors\":\"Amy Eckland, Michael Kohut, Henry Stoddard, Deb Burris, Frank Chessa, Monica K Sikka, Daniel A Solomon, Colleen M Kershaw, Ellen F Eaton, Rebecca Hutchinson, Peter D Friedmann, Thomas J Stopka, Kathleen M Fairfield, Kinna Thakarar\",\"doi\":\"10.1177/20499361231197065\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>People who inject drugs (PWID) are at risk for severe bacterial and fungal infections including skin and soft tissue infections, endocarditis, and osteomyelitis. PWID have high rates of self-directed discharge and are often not offered outpatient antimicrobial therapies, despite studies showing their efficacy and safety in PWID. This study fills a gap in knowledge of patient and community partner perspectives on treatment and discharge decision making for injection drug use (IDU)-associated infections.</p><p><strong>Methods: </strong>We conducted semi-structured interviews with patients (<i>n</i> = 10) hospitalized with IDU-associated infections and community partners (<i>n</i> = 6) in the Portland, Maine region. Community partners include peer support workers at syringe services programs (SSPs) and outreach specialists working with PWID. We transcribed and thematically analyzed interviews to explore perspectives on three domains: perspectives on long-term hospitalization, outpatient treatment options, and patient involvement in decision making.</p><p><strong>Results: </strong>Participants noted that stigma and inadequate pain management created poor hospitalization experiences that contributed to self-directed discharge. On the other hand, patients reported hospitalization provided opportunities to connect to substance use disorder (SUD) treatment and protect them from outside substance use triggers. Many patients expressed interest in outpatient antimicrobial treatment options conditional upon perceived efficacy of the treatment, perceived ability to complete treatment, and available resources and social support. Finally, both patients and community partners emphasized the importance of autonomy and inclusion in medical decision making. Although some participants acknowledged their SUD, withdrawal symptoms, or undertreated pain might interfere with decision making, they felt these medical conditions were not justification for health care professionals withholding treatment options. They recommended open communication to build trust and reduce harms.</p><p><strong>Conclusion: </strong>Patients with IDU-associated infections desire autonomy, respect, and patient-centered care from healthcare workers, and may self-discharge when needs or preferences are not met. Involving patients in treatment decisions and offering outpatient antimicrobial options may result in better outcomes. However, patient involvement in decision making may be complicated by many contextual factors unique to each patient, suggesting a need for shared decision making to meet the needs of hospitalized patients with IDU-associated infections.</p>\",\"PeriodicalId\":46154,\"journal\":{\"name\":\"Therapeutic Advances in Infectious Disease\",\"volume\":\"10 \",\"pages\":\"20499361231197065\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/f6/10.1177_20499361231197065.PMC10492466.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Infectious Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20499361231197065\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Infectious Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20499361231197065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
"I know my body better than anyone else": a qualitative study of perspectives of people with lived experience on antimicrobial treatment decisions for injection drug use-associated infections.
Background: People who inject drugs (PWID) are at risk for severe bacterial and fungal infections including skin and soft tissue infections, endocarditis, and osteomyelitis. PWID have high rates of self-directed discharge and are often not offered outpatient antimicrobial therapies, despite studies showing their efficacy and safety in PWID. This study fills a gap in knowledge of patient and community partner perspectives on treatment and discharge decision making for injection drug use (IDU)-associated infections.
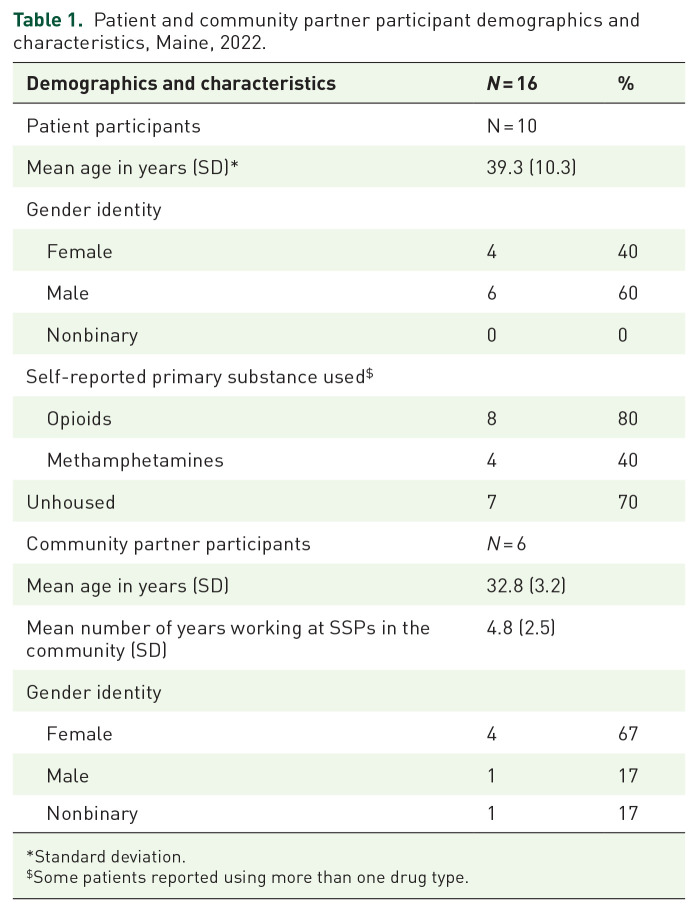
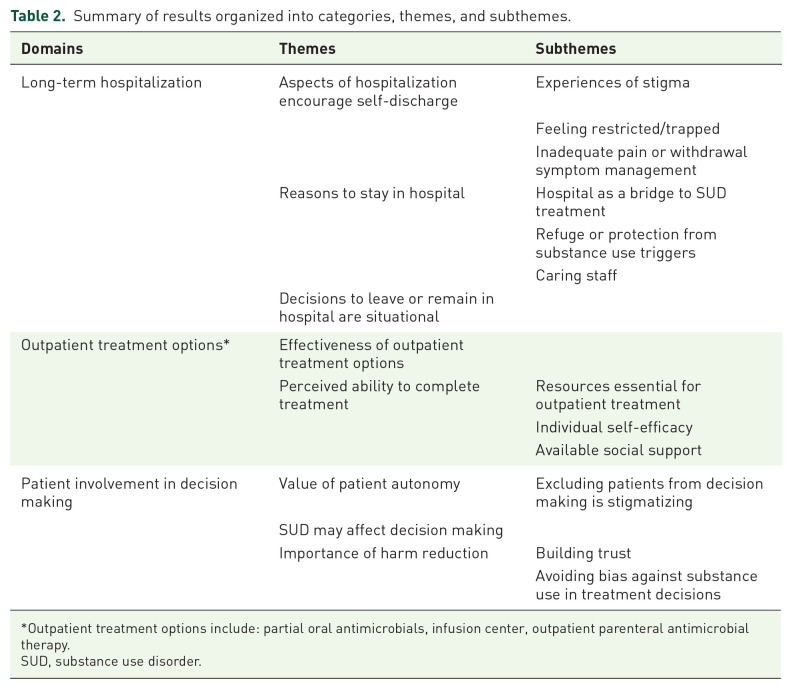
Methods: We conducted semi-structured interviews with patients (n = 10) hospitalized with IDU-associated infections and community partners (n = 6) in the Portland, Maine region. Community partners include peer support workers at syringe services programs (SSPs) and outreach specialists working with PWID. We transcribed and thematically analyzed interviews to explore perspectives on three domains: perspectives on long-term hospitalization, outpatient treatment options, and patient involvement in decision making.
Results: Participants noted that stigma and inadequate pain management created poor hospitalization experiences that contributed to self-directed discharge. On the other hand, patients reported hospitalization provided opportunities to connect to substance use disorder (SUD) treatment and protect them from outside substance use triggers. Many patients expressed interest in outpatient antimicrobial treatment options conditional upon perceived efficacy of the treatment, perceived ability to complete treatment, and available resources and social support. Finally, both patients and community partners emphasized the importance of autonomy and inclusion in medical decision making. Although some participants acknowledged their SUD, withdrawal symptoms, or undertreated pain might interfere with decision making, they felt these medical conditions were not justification for health care professionals withholding treatment options. They recommended open communication to build trust and reduce harms.
Conclusion: Patients with IDU-associated infections desire autonomy, respect, and patient-centered care from healthcare workers, and may self-discharge when needs or preferences are not met. Involving patients in treatment decisions and offering outpatient antimicrobial options may result in better outcomes. However, patient involvement in decision making may be complicated by many contextual factors unique to each patient, suggesting a need for shared decision making to meet the needs of hospitalized patients with IDU-associated infections.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
