T R Zaat, E B Kostova, P Korsen, M G Showell, F Mol, M van Wely
{"title":"自然与人工周期冷冻胚胎移植后的产科和新生儿结局以及黄体期支持的作用:一项系统回顾和荟萃分析","authors":"T R Zaat, E B Kostova, P Korsen, M G Showell, F Mol, M van Wely","doi":"10.1093/humupd/dmad011","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The number of frozen embryo transfers (FET) has increased dramatically over the past decade. Based on current evidence, there is no difference in pregnancy rates when natural cycle FET (NC-FET) is compared to artificial cycle FET (AC-FET) in subfertile women. However, NC-FET seems to be associated with lower risk of adverse obstetric and neonatal outcomes compared with AC-FET cycles. Currently, there is no consensus about whether NC-FET needs to be combined with luteal phase support (LPS) or not. The question of how to prepare the endometrium for FET has now gained even more importance and taken the dimension of safety into account as it should not simply be reduced to the basic question of effectiveness.</p><p><strong>Objective and rationale: </strong>The objective of this project was to determine whether NC-FET, with or without LPS, decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET.</p><p><strong>Search methods: </strong>A systematic review and meta-analysis was carried out. A literature search was performed using the following databases: CINAHL, EMBASE, and MEDLINE from inception to 10 October 2022. Observational studies, including cohort studies, and registries comparing obstetric and neonatal outcomes between singleton pregnancies after NC-FET and those after AC-FET were sought. Risk of bias was assessed using the ROBINS-I tool. The quality of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation approach. We calculated pooled odds ratios (ORs), pooled risk differences (RDs), pooled adjusted ORs, and prevalence estimates with 95% CI using a random effect model, while heterogeneity was assessed by the I2.</p><p><strong>Outcomes: </strong>The conducted search identified 2436 studies, 890 duplicates were removed and 1546 studies were screened. Thirty studies (NC-FET n = 56 445; AC-FET n = 57 231) were included, 19 of which used LPS in NC-FET. Birthweight was lower following NC-FET versus AC-FET (mean difference 26.35 g; 95% CI 11.61-41.08, I2 = 63%). Furthermore NC-FET compared to AC-FET resulted in a lower risk of large for gestational age (OR 0.88, 95% 0.83-0.94, I2 = 54%), macrosomia (OR 0.81; 95% CI 0.71-0.93, I2 = 68%), low birthweight (OR 0.81, 95% CI 0.77-0.85, I2 = 41%), early pregnancy loss (OR 0.73; 95% CI 0.61-0.86, I2 = 70%), preterm birth (OR 0.80; 95% CI 0.75-0.85, I2 = 20%), very preterm birth (OR 0.66, 95% CI 0.53-0.84, I2 = 0%), hypertensive disorders of pregnancy (OR 0.60, 95% CI 0.50-0.65, I2 = 61%), pre-eclampsia (OR 0.50; 95% CI 0.42-0.60, I2 = 44%), placenta previa (OR 0.84, 95% CI 0.73-0.97, I2 = 0%), and postpartum hemorrhage (OR 0.43; 95% CI 0.38-0.48, I2 = 53%). Stratified analyses on LPS use in NC-FET suggested that, compared to AC-FET, NC-FET with LPS decreased preterm birth risk, while NC-FET without LPS did not (OR 0.75, 95% CI 0.70-0.81). LPS use did not modify the other outcomes. Heterogeneity varied from low to high, while quality of the evidence was very low to moderate.</p><p><strong>Wider implications: </strong>This study confirms that NC-FET decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET. We estimate that for each adverse outcome, use of NC-FET may prevent 4 to 22 cases per 1000 women. Consequently, NC-FET should be the preferred treatment in women with ovulatory cycles undergoing FET. Based on very low quality of evidence, the risk of preterm birth be decreased when LPS is used in NC-FET compared to AC-FET. However, because of many uncertainties-the major being the debate about efficacy of the use of LPS-future research is needed on efficacy and safety of LPS and no recommendation can be made about the use of LPS.</p>","PeriodicalId":55045,"journal":{"name":"Human Reproduction Update","volume":"29 5","pages":"634-654"},"PeriodicalIF":16.1000,"publicationDate":"2023-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/93/dmad011.PMC10477943.pdf","citationCount":"5","resultStr":"{\"title\":\"Obstetric and neonatal outcomes after natural versus artificial cycle frozen embryo transfer and the role of luteal phase support: a systematic review and meta-analysis.\",\"authors\":\"T R Zaat, E B Kostova, P Korsen, M G Showell, F Mol, M van Wely\",\"doi\":\"10.1093/humupd/dmad011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The number of frozen embryo transfers (FET) has increased dramatically over the past decade. Based on current evidence, there is no difference in pregnancy rates when natural cycle FET (NC-FET) is compared to artificial cycle FET (AC-FET) in subfertile women. However, NC-FET seems to be associated with lower risk of adverse obstetric and neonatal outcomes compared with AC-FET cycles. Currently, there is no consensus about whether NC-FET needs to be combined with luteal phase support (LPS) or not. The question of how to prepare the endometrium for FET has now gained even more importance and taken the dimension of safety into account as it should not simply be reduced to the basic question of effectiveness.</p><p><strong>Objective and rationale: </strong>The objective of this project was to determine whether NC-FET, with or without LPS, decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET.</p><p><strong>Search methods: </strong>A systematic review and meta-analysis was carried out. A literature search was performed using the following databases: CINAHL, EMBASE, and MEDLINE from inception to 10 October 2022. Observational studies, including cohort studies, and registries comparing obstetric and neonatal outcomes between singleton pregnancies after NC-FET and those after AC-FET were sought. Risk of bias was assessed using the ROBINS-I tool. The quality of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation approach. We calculated pooled odds ratios (ORs), pooled risk differences (RDs), pooled adjusted ORs, and prevalence estimates with 95% CI using a random effect model, while heterogeneity was assessed by the I2.</p><p><strong>Outcomes: </strong>The conducted search identified 2436 studies, 890 duplicates were removed and 1546 studies were screened. Thirty studies (NC-FET n = 56 445; AC-FET n = 57 231) were included, 19 of which used LPS in NC-FET. Birthweight was lower following NC-FET versus AC-FET (mean difference 26.35 g; 95% CI 11.61-41.08, I2 = 63%). Furthermore NC-FET compared to AC-FET resulted in a lower risk of large for gestational age (OR 0.88, 95% 0.83-0.94, I2 = 54%), macrosomia (OR 0.81; 95% CI 0.71-0.93, I2 = 68%), low birthweight (OR 0.81, 95% CI 0.77-0.85, I2 = 41%), early pregnancy loss (OR 0.73; 95% CI 0.61-0.86, I2 = 70%), preterm birth (OR 0.80; 95% CI 0.75-0.85, I2 = 20%), very preterm birth (OR 0.66, 95% CI 0.53-0.84, I2 = 0%), hypertensive disorders of pregnancy (OR 0.60, 95% CI 0.50-0.65, I2 = 61%), pre-eclampsia (OR 0.50; 95% CI 0.42-0.60, I2 = 44%), placenta previa (OR 0.84, 95% CI 0.73-0.97, I2 = 0%), and postpartum hemorrhage (OR 0.43; 95% CI 0.38-0.48, I2 = 53%). Stratified analyses on LPS use in NC-FET suggested that, compared to AC-FET, NC-FET with LPS decreased preterm birth risk, while NC-FET without LPS did not (OR 0.75, 95% CI 0.70-0.81). LPS use did not modify the other outcomes. Heterogeneity varied from low to high, while quality of the evidence was very low to moderate.</p><p><strong>Wider implications: </strong>This study confirms that NC-FET decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET. We estimate that for each adverse outcome, use of NC-FET may prevent 4 to 22 cases per 1000 women. Consequently, NC-FET should be the preferred treatment in women with ovulatory cycles undergoing FET. Based on very low quality of evidence, the risk of preterm birth be decreased when LPS is used in NC-FET compared to AC-FET. However, because of many uncertainties-the major being the debate about efficacy of the use of LPS-future research is needed on efficacy and safety of LPS and no recommendation can be made about the use of LPS.</p>\",\"PeriodicalId\":55045,\"journal\":{\"name\":\"Human Reproduction Update\",\"volume\":\"29 5\",\"pages\":\"634-654\"},\"PeriodicalIF\":16.1000,\"publicationDate\":\"2023-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/93/dmad011.PMC10477943.pdf\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human Reproduction Update\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/humupd/dmad011\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human Reproduction Update","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/humupd/dmad011","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 5
摘要
背景:在过去的十年中,冷冻胚胎移植(FET)的数量急剧增加。根据目前的证据,在低生育能力妇女中,自然周期FET (NC-FET)与人工周期FET (AC-FET)相比,妊娠率没有差异。然而,与AC-FET周期相比,NC-FET似乎与较低的不良产科和新生儿结局风险相关。目前,对于NC-FET是否需要与黄体期支持(LPS)联合使用,尚未达成共识。如何为FET准备子宫内膜的问题现在变得更加重要,并考虑到安全方面,因为它不应简单地简化为有效性的基本问题。目的和理由:该项目的目的是确定与AC-FET相比,NC-FET在加或不加LPS的情况下是否降低了产科和新生儿不良结局的风险。检索方法:进行系统综述和荟萃分析。使用以下数据库进行文献检索:CINAHL、EMBASE和MEDLINE,检索时间为成立至2022年10月10日。观察性研究,包括队列研究,以及比较NC-FET和AC-FET后单胎妊娠的产科和新生儿结局的登记。使用ROBINS-I工具评估偏倚风险。采用建议分级评估、发展和评价方法评价证据质量。我们使用随机效应模型计算合并优势比(or)、合并风险差异(RDs)、合并调整后的or和95% CI的患病率估计值,同时通过I2评估异质性。结果:进行的检索确定了2436项研究,删除了890项重复,筛选了1546项研究。30项研究(NC-FET n = 56 445;共纳入AC-FET (n = 57 231),其中19例采用LPS处理NC-FET。与AC-FET相比,NC-FET的出生体重更低(平均差26.35 g;95% ci 11.61-41.08, i2 = 63%)。此外,与AC-FET相比,NC-FET导致大胎龄(OR 0.88, 95% 0.83-0.94, I2 = 54%)、巨大儿(OR 0.81;95% CI 0.71-0.93, I2 = 68%),低出生体重(OR 0.81, 95% CI 0.77-0.85, I2 = 41%),早孕丢失(OR 0.73;95% CI 0.61-0.86, I2 = 70%),早产(OR 0.80;95% CI 0.75-0.85, I2 = 20%),重度早产(OR 0.66, 95% CI 0.53-0.84, I2 = 0%),妊娠期高血压疾病(OR 0.60, 95% CI 0.50-0.65, I2 = 61%),先兆子痫(OR 0.50;95% CI 0.42-0.60, I2 = 44%)、前置胎盘(OR 0.84, 95% CI 0.73-0.97, I2 = 0%)和产后出血(OR 0.43;95% ci 0.38-0.48, i2 = 53%)。对LPS在NC-FET中使用的分层分析表明,与AC-FET相比,LPS的NC-FET降低了早产风险,而不使用LPS的NC-FET则没有(OR 0.75, 95% CI 0.70-0.81)。LPS的使用没有改变其他结果。异质性从低到高,证据质量从极低到中等。更广泛的影响:本研究证实,与AC-FET相比,NC-FET降低了不良产科和新生儿结局的风险。我们估计,对于每一种不良后果,使用NC-FET可预防每1000名妇女4至22例。因此,NC-FET应该是排卵周期接受FET的女性的首选治疗方法。基于非常低质量的证据,与AC-FET相比,在NC-FET中使用LPS可降低早产风险。然而,由于存在许多不确定性,主要是关于脂多糖使用的有效性的争论,因此需要对脂多糖的有效性和安全性进行进一步的研究,目前还不能对脂多糖的使用提出建议。
Obstetric and neonatal outcomes after natural versus artificial cycle frozen embryo transfer and the role of luteal phase support: a systematic review and meta-analysis.
Background: The number of frozen embryo transfers (FET) has increased dramatically over the past decade. Based on current evidence, there is no difference in pregnancy rates when natural cycle FET (NC-FET) is compared to artificial cycle FET (AC-FET) in subfertile women. However, NC-FET seems to be associated with lower risk of adverse obstetric and neonatal outcomes compared with AC-FET cycles. Currently, there is no consensus about whether NC-FET needs to be combined with luteal phase support (LPS) or not. The question of how to prepare the endometrium for FET has now gained even more importance and taken the dimension of safety into account as it should not simply be reduced to the basic question of effectiveness.
Objective and rationale: The objective of this project was to determine whether NC-FET, with or without LPS, decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET.
Search methods: A systematic review and meta-analysis was carried out. A literature search was performed using the following databases: CINAHL, EMBASE, and MEDLINE from inception to 10 October 2022. Observational studies, including cohort studies, and registries comparing obstetric and neonatal outcomes between singleton pregnancies after NC-FET and those after AC-FET were sought. Risk of bias was assessed using the ROBINS-I tool. The quality of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation approach. We calculated pooled odds ratios (ORs), pooled risk differences (RDs), pooled adjusted ORs, and prevalence estimates with 95% CI using a random effect model, while heterogeneity was assessed by the I2.
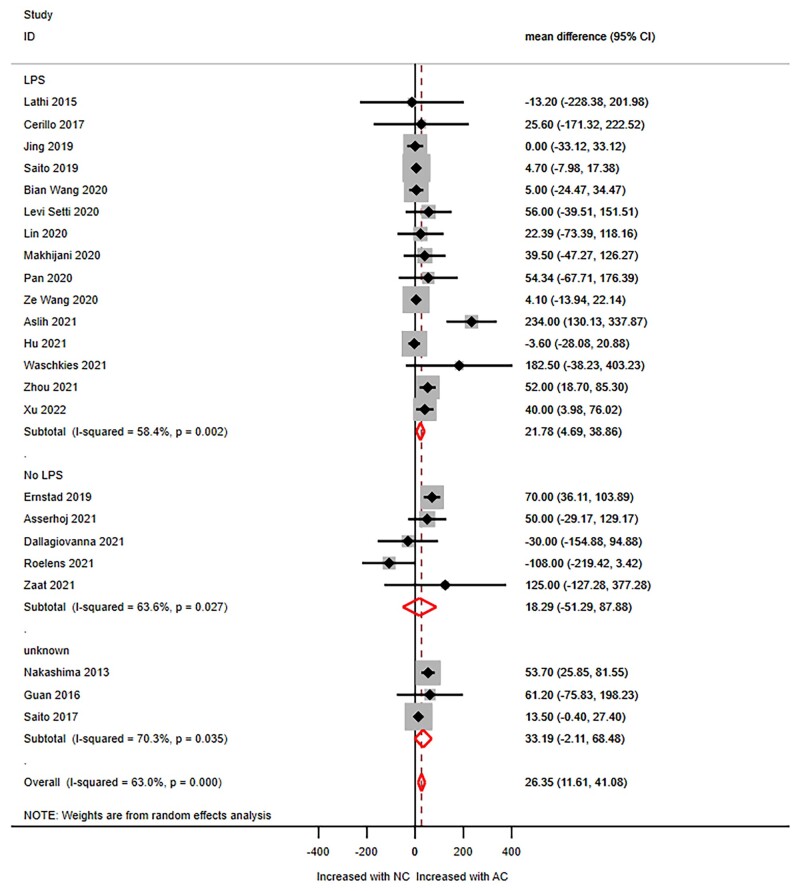
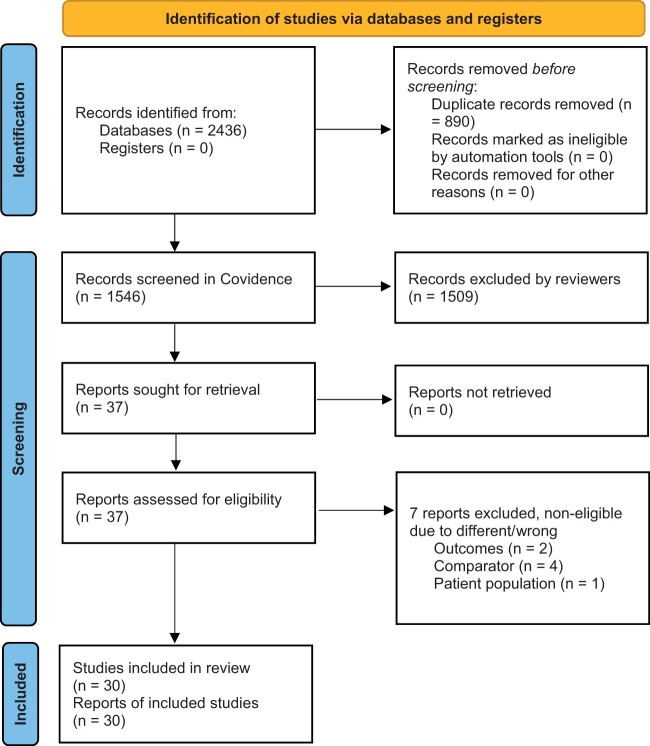
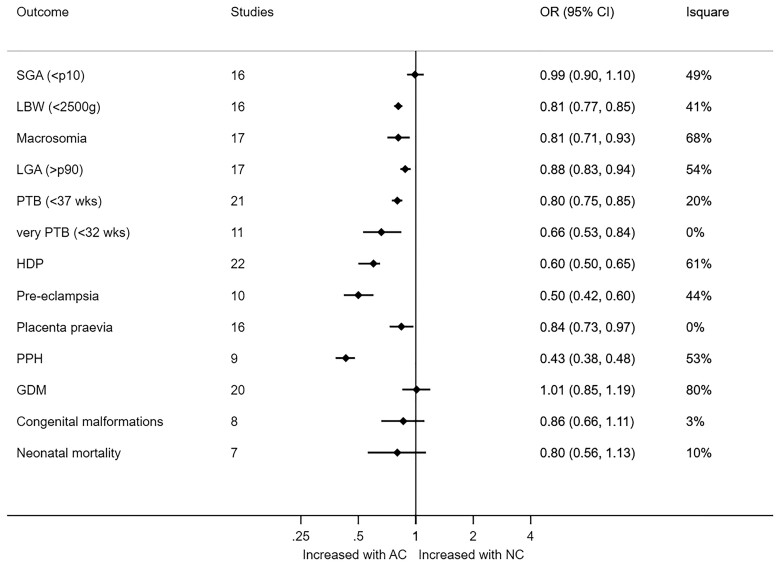
Outcomes: The conducted search identified 2436 studies, 890 duplicates were removed and 1546 studies were screened. Thirty studies (NC-FET n = 56 445; AC-FET n = 57 231) were included, 19 of which used LPS in NC-FET. Birthweight was lower following NC-FET versus AC-FET (mean difference 26.35 g; 95% CI 11.61-41.08, I2 = 63%). Furthermore NC-FET compared to AC-FET resulted in a lower risk of large for gestational age (OR 0.88, 95% 0.83-0.94, I2 = 54%), macrosomia (OR 0.81; 95% CI 0.71-0.93, I2 = 68%), low birthweight (OR 0.81, 95% CI 0.77-0.85, I2 = 41%), early pregnancy loss (OR 0.73; 95% CI 0.61-0.86, I2 = 70%), preterm birth (OR 0.80; 95% CI 0.75-0.85, I2 = 20%), very preterm birth (OR 0.66, 95% CI 0.53-0.84, I2 = 0%), hypertensive disorders of pregnancy (OR 0.60, 95% CI 0.50-0.65, I2 = 61%), pre-eclampsia (OR 0.50; 95% CI 0.42-0.60, I2 = 44%), placenta previa (OR 0.84, 95% CI 0.73-0.97, I2 = 0%), and postpartum hemorrhage (OR 0.43; 95% CI 0.38-0.48, I2 = 53%). Stratified analyses on LPS use in NC-FET suggested that, compared to AC-FET, NC-FET with LPS decreased preterm birth risk, while NC-FET without LPS did not (OR 0.75, 95% CI 0.70-0.81). LPS use did not modify the other outcomes. Heterogeneity varied from low to high, while quality of the evidence was very low to moderate.
Wider implications: This study confirms that NC-FET decreases the risk of adverse obstetric and neonatal outcomes compared with AC-FET. We estimate that for each adverse outcome, use of NC-FET may prevent 4 to 22 cases per 1000 women. Consequently, NC-FET should be the preferred treatment in women with ovulatory cycles undergoing FET. Based on very low quality of evidence, the risk of preterm birth be decreased when LPS is used in NC-FET compared to AC-FET. However, because of many uncertainties-the major being the debate about efficacy of the use of LPS-future research is needed on efficacy and safety of LPS and no recommendation can be made about the use of LPS.
期刊介绍:
Human Reproduction Update is the leading journal in its field, boasting a Journal Impact FactorTM of 13.3 and ranked first in Obstetrics & Gynecology and Reproductive Biology (Source: Journal Citation ReportsTM from Clarivate, 2023). It specializes in publishing comprehensive and systematic review articles covering various aspects of human reproductive physiology and medicine.
The journal prioritizes basic, transitional, and clinical topics related to reproduction, encompassing areas such as andrology, embryology, infertility, gynaecology, pregnancy, reproductive endocrinology, reproductive epidemiology, reproductive genetics, reproductive immunology, and reproductive oncology. Human Reproduction Update is published on behalf of the European Society of Human Reproduction and Embryology (ESHRE), maintaining the highest scientific and editorial standards.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
