Matthew A Remz, Joshua K Wong, Justin D Hilliard, Tracy Tholanikunnel, Ashley E Rawls, Michael S Okun
{"title":"与STN DBS相关的持续性刺激诱导运动障碍的识别和管理:跷跷板困境。","authors":"Matthew A Remz, Joshua K Wong, Justin D Hilliard, Tracy Tholanikunnel, Ashley E Rawls, Michael S Okun","doi":"10.5334/tohm.780","DOIUrl":null,"url":null,"abstract":"<p><strong>Clinical vignette: </strong>A 73-year-old woman with Parkinson's disease (PD) underwent implantation of bilateral subthalamic nucleus deep brain stimulators (STN-DBS) to address bilateral upper extremity medication-refractory tremor. Post-operatively, she experienced a \"see-saw effect\" where small increases in stimulation resulted in improvement in one symptom (tremor) with concurrent worsening in another (dyskinesia).</p><p><strong>Clinical dilemma: </strong>SID is usually considered a positive predictor of DBS outcome. However, there are cases where SID cannot be optimized. Lead location and pre-operative characteristics may contribute to this adverse effect. If the combination of programming and medication adjustments fails to resolve SID, what can be done to \"rescue\" the outcome?</p><p><strong>Clinical solution: </strong>Management of SID requires a gradual and steadfast programming approach. Post-operative lead localization can guide advanced programming and decision-making. Rescue surgical interventions may be considered.</p><p><strong>Gap in knowledge: </strong>In cases where SID is persistent despite deploying persistent optimization strategies, there is limited guidance on next steps.</p>","PeriodicalId":23317,"journal":{"name":"Tremor and Other Hyperkinetic Movements","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10473163/pdf/","citationCount":"1","resultStr":"{\"title\":\"Identification and Management of Persistent Stimulation-Induced Dyskinesia Associated with STN DBS: The See-Saw Dilemma.\",\"authors\":\"Matthew A Remz, Joshua K Wong, Justin D Hilliard, Tracy Tholanikunnel, Ashley E Rawls, Michael S Okun\",\"doi\":\"10.5334/tohm.780\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Clinical vignette: </strong>A 73-year-old woman with Parkinson's disease (PD) underwent implantation of bilateral subthalamic nucleus deep brain stimulators (STN-DBS) to address bilateral upper extremity medication-refractory tremor. Post-operatively, she experienced a \\\"see-saw effect\\\" where small increases in stimulation resulted in improvement in one symptom (tremor) with concurrent worsening in another (dyskinesia).</p><p><strong>Clinical dilemma: </strong>SID is usually considered a positive predictor of DBS outcome. However, there are cases where SID cannot be optimized. Lead location and pre-operative characteristics may contribute to this adverse effect. If the combination of programming and medication adjustments fails to resolve SID, what can be done to \\\"rescue\\\" the outcome?</p><p><strong>Clinical solution: </strong>Management of SID requires a gradual and steadfast programming approach. Post-operative lead localization can guide advanced programming and decision-making. Rescue surgical interventions may be considered.</p><p><strong>Gap in knowledge: </strong>In cases where SID is persistent despite deploying persistent optimization strategies, there is limited guidance on next steps.</p>\",\"PeriodicalId\":23317,\"journal\":{\"name\":\"Tremor and Other Hyperkinetic Movements\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10473163/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tremor and Other Hyperkinetic Movements\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5334/tohm.780\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tremor and Other Hyperkinetic Movements","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/tohm.780","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Identification and Management of Persistent Stimulation-Induced Dyskinesia Associated with STN DBS: The See-Saw Dilemma.
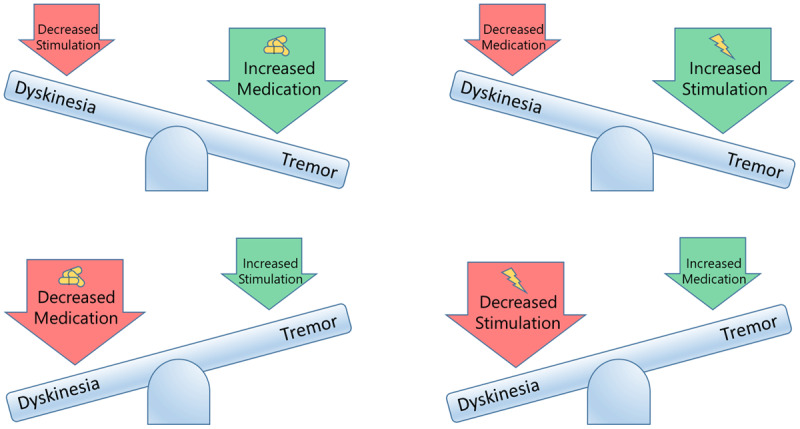
Clinical vignette: A 73-year-old woman with Parkinson's disease (PD) underwent implantation of bilateral subthalamic nucleus deep brain stimulators (STN-DBS) to address bilateral upper extremity medication-refractory tremor. Post-operatively, she experienced a "see-saw effect" where small increases in stimulation resulted in improvement in one symptom (tremor) with concurrent worsening in another (dyskinesia).
Clinical dilemma: SID is usually considered a positive predictor of DBS outcome. However, there are cases where SID cannot be optimized. Lead location and pre-operative characteristics may contribute to this adverse effect. If the combination of programming and medication adjustments fails to resolve SID, what can be done to "rescue" the outcome?
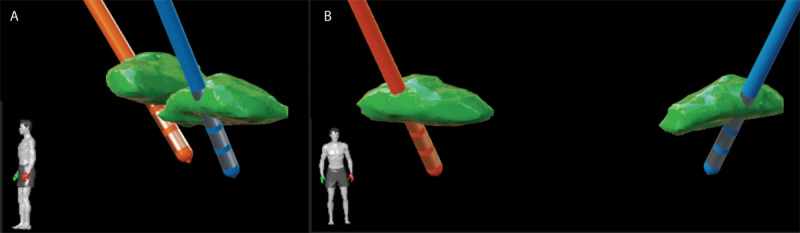
Clinical solution: Management of SID requires a gradual and steadfast programming approach. Post-operative lead localization can guide advanced programming and decision-making. Rescue surgical interventions may be considered.
Gap in knowledge: In cases where SID is persistent despite deploying persistent optimization strategies, there is limited guidance on next steps.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
