Khawaja Afzal Ammar MD, MS, Richard J. Rodeheffer MD
{"title":"重新评估心电图未识别心肌梗死的临床意义:放射性核素梗死大小及其对长期预后的影响","authors":"Khawaja Afzal Ammar MD, MS, Richard J. Rodeheffer MD","doi":"10.1111/anec.13088","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Silent or unrecognized myocardial infarction (UMI) diagnosed by surveillance electrocardiography (ECG) carries similarly poor prognosis as recognized MI (RMI) for poorly understood reasons.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study included 5430 consecutive patients who presented to the nuclear laboratory and underwent 2-day stress and rest Tc-<sup>99m</sup> sestamibi and ECG studies between March 1991 and June 1999. UMI was diagnosed if ECG showed <i>Q</i>-wave MI in the absence of a history of RMI. We measured infarct size (% defect size as compared with the entire left ventricular sestamibi uptake), ejection fraction (EF, %), and summed difference score (SDS, sestamibi uptake by myocardium in stress minus sestamibi uptake in rest images as a marker of ischemia). Survival was determined by follow-up survey (median 6 years).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We identified 346 UMIs, 628 RMIs, and 4456 subjects without MI (No MI). As compared with RMI, UMI patients had lesser abnormalities on nuclear scans (<i>p</i> < .0001 for all), including smaller infarct size (5.7% vs. 12.2%), higher EF (58% vs. 53%), and lesser ischemia (SDS; 3.9% vs. 2.7%). UMI prognosis was as poor as that of RMI (annual mortality rate 4.7% vs. 4.8% with No MI rate of 2.9%; <i>p</i> < .001 for all comparisons), and this persisted after multivariate analysis. Infarct size quantification successfully risk-stratified ECG-UMI patients, but UMI patients continued to predict mortality even if the infarct size was 0%.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Although UMI patients have lesser abnormalities on nuclear scans, ECG-based UMI continues to independently predict mortality, indicating the continuing relevance of ECG in clinical practice.</p>\n </section>\n </div>","PeriodicalId":8074,"journal":{"name":"Annals of Noninvasive Electrocardiology","volume":"28 6","pages":""},"PeriodicalIF":1.1000,"publicationDate":"2023-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anec.13088","citationCount":"0","resultStr":"{\"title\":\"Reassessing the clinical significance of electrocardiographically unrecognized myocardial infarctions: Radionuclide infarct size and its impact on long-term prognosis\",\"authors\":\"Khawaja Afzal Ammar MD, MS, Richard J. Rodeheffer MD\",\"doi\":\"10.1111/anec.13088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Silent or unrecognized myocardial infarction (UMI) diagnosed by surveillance electrocardiography (ECG) carries similarly poor prognosis as recognized MI (RMI) for poorly understood reasons.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This study included 5430 consecutive patients who presented to the nuclear laboratory and underwent 2-day stress and rest Tc-<sup>99m</sup> sestamibi and ECG studies between March 1991 and June 1999. UMI was diagnosed if ECG showed <i>Q</i>-wave MI in the absence of a history of RMI. We measured infarct size (% defect size as compared with the entire left ventricular sestamibi uptake), ejection fraction (EF, %), and summed difference score (SDS, sestamibi uptake by myocardium in stress minus sestamibi uptake in rest images as a marker of ischemia). Survival was determined by follow-up survey (median 6 years).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We identified 346 UMIs, 628 RMIs, and 4456 subjects without MI (No MI). As compared with RMI, UMI patients had lesser abnormalities on nuclear scans (<i>p</i> < .0001 for all), including smaller infarct size (5.7% vs. 12.2%), higher EF (58% vs. 53%), and lesser ischemia (SDS; 3.9% vs. 2.7%). UMI prognosis was as poor as that of RMI (annual mortality rate 4.7% vs. 4.8% with No MI rate of 2.9%; <i>p</i> < .001 for all comparisons), and this persisted after multivariate analysis. Infarct size quantification successfully risk-stratified ECG-UMI patients, but UMI patients continued to predict mortality even if the infarct size was 0%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Although UMI patients have lesser abnormalities on nuclear scans, ECG-based UMI continues to independently predict mortality, indicating the continuing relevance of ECG in clinical practice.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8074,\"journal\":{\"name\":\"Annals of Noninvasive Electrocardiology\",\"volume\":\"28 6\",\"pages\":\"\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2023-09-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anec.13088\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Noninvasive Electrocardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/anec.13088\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Noninvasive Electrocardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anec.13088","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
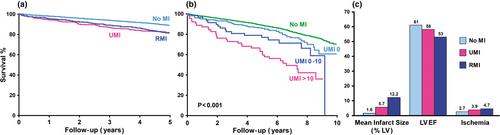
背景:监测心电图(ECG)诊断的无症状或无法识别的心肌梗死(UMI)与已识别的心肌梗死(RMI)有着相似的不良预后,原因尚不清楚。方法在1991年3月至1999年6月期间,5430例连续到核实验室就诊的患者进行了为期2天的应激休息Tc-99m sestamibi和心电图检查。在没有RMI病史的情况下,如果心电图显示q波MI,则诊断为UMI。我们测量了梗死面积(缺损面积与整个左心室安定比摄取的百分比)、射血分数(EF, %)和总差异评分(SDS,应激状态下心肌安定比摄取减去静止状态下安定比摄取作为缺血标志)。生存率通过随访调查确定(中位6年)。结果我们确定了346名UMIs, 628名RMIs和4456名无MI (No MI)的受试者。与RMI相比,UMI患者在核扫描上的异常较少(p <)。0001),包括较小的梗死面积(5.7%对12.2%),较高的EF(58%对53%)和较小的缺血(SDS;3.9% vs. 2.7%)。UMI预后与RMI一样差(年死亡率4.7% vs. 4.8%,无MI率2.9%;p <001),在多变量分析后,这种情况仍然存在。梗死面积量化成功地对ECG-UMI患者进行了风险分层,但即使梗死面积为0%,UMI患者仍能预测死亡率。尽管UMI患者在核扫描上的异常较小,但基于ECG的UMI仍然可以独立预测死亡率,这表明ECG在临床实践中仍然具有相关性。
Reassessing the clinical significance of electrocardiographically unrecognized myocardial infarctions: Radionuclide infarct size and its impact on long-term prognosis
Background
Silent or unrecognized myocardial infarction (UMI) diagnosed by surveillance electrocardiography (ECG) carries similarly poor prognosis as recognized MI (RMI) for poorly understood reasons.
Methods
This study included 5430 consecutive patients who presented to the nuclear laboratory and underwent 2-day stress and rest Tc-99m sestamibi and ECG studies between March 1991 and June 1999. UMI was diagnosed if ECG showed Q-wave MI in the absence of a history of RMI. We measured infarct size (% defect size as compared with the entire left ventricular sestamibi uptake), ejection fraction (EF, %), and summed difference score (SDS, sestamibi uptake by myocardium in stress minus sestamibi uptake in rest images as a marker of ischemia). Survival was determined by follow-up survey (median 6 years).
Results
We identified 346 UMIs, 628 RMIs, and 4456 subjects without MI (No MI). As compared with RMI, UMI patients had lesser abnormalities on nuclear scans (p < .0001 for all), including smaller infarct size (5.7% vs. 12.2%), higher EF (58% vs. 53%), and lesser ischemia (SDS; 3.9% vs. 2.7%). UMI prognosis was as poor as that of RMI (annual mortality rate 4.7% vs. 4.8% with No MI rate of 2.9%; p < .001 for all comparisons), and this persisted after multivariate analysis. Infarct size quantification successfully risk-stratified ECG-UMI patients, but UMI patients continued to predict mortality even if the infarct size was 0%.
Conclusions
Although UMI patients have lesser abnormalities on nuclear scans, ECG-based UMI continues to independently predict mortality, indicating the continuing relevance of ECG in clinical practice.
期刊介绍:
The ANNALS OF NONINVASIVE ELECTROCARDIOLOGY (A.N.E) is an online only journal that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients.
ANE is the first journal in an evolving subspecialty that incorporates ongoing advances in the clinical application and technology of traditional and new ECG-based techniques in the diagnosis and treatment of cardiac patients. The publication includes topics related to 12-lead, exercise and high-resolution electrocardiography, arrhythmias, ischemia, repolarization phenomena, heart rate variability, circadian rhythms, bioengineering technology, signal-averaged ECGs, T-wave alternans and automatic external defibrillation.
ANE publishes peer-reviewed articles of interest to clinicians and researchers in the field of noninvasive electrocardiology. Original research, clinical studies, state-of-the-art reviews, case reports, technical notes, and letters to the editors will be published to meet future demands in this field.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
