Brian De, Rituraj Upadhyay, Kaiping Liao, Tiffany Kumala, Christopher Shi, Grace Dodoo, Joseph Abi Jaoude, Kelsey L Corrigan, Gohar S Manzar, Kathryn E Marqueen, Vincent Bernard, Sunyoung S Lee, Kanwal P S Raghav, Jean-Nicolas Vauthey, Ching-Wei D Tzeng, Hop S Tran Cao, Grace Lee, Jennifer Y Wo, Theodore S Hong, Christopher H Crane, Bruce D Minsky, Grace L Smith, Emma B Holliday, Cullen M Taniguchi, Albert C Koong, Prajnan Das, Milind Javle, Ethan B Ludmir, Eugene J Koay
{"title":"肝内胆管癌肝外转移的明确肝放射治疗。","authors":"Brian De, Rituraj Upadhyay, Kaiping Liao, Tiffany Kumala, Christopher Shi, Grace Dodoo, Joseph Abi Jaoude, Kelsey L Corrigan, Gohar S Manzar, Kathryn E Marqueen, Vincent Bernard, Sunyoung S Lee, Kanwal P S Raghav, Jean-Nicolas Vauthey, Ching-Wei D Tzeng, Hop S Tran Cao, Grace Lee, Jennifer Y Wo, Theodore S Hong, Christopher H Crane, Bruce D Minsky, Grace L Smith, Emma B Holliday, Cullen M Taniguchi, Albert C Koong, Prajnan Das, Milind Javle, Ethan B Ludmir, Eugene J Koay","doi":"10.1159/000530134","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Tumor-related liver failure (TRLF) is the most common cause of death in patients with intrahepatic cholangiocarcinoma (ICC). Though we previously showed that liver radiotherapy (L-RT) for locally advanced ICC is associated with less frequent TRLF and longer overall survival (OS), the role of L-RT for patients with extrahepatic metastatic disease (M1) remains undefined. We sought to compare outcomes for M1 ICC patients treated with and without L-RT.</p><p><strong>Methods: </strong>We reviewed ICC patients that found to have M1 disease at initial diagnosis at a single institution between 2010 and 2021 who received L-RT, matching them with an institutional cohort by propensity score and a National Cancer Database (NCDB) cohort by frequency technique. The median biologically effective dose was 97.5 Gy (interquartile range 80.5-97.9 Gy) for L-RT. Patients treated with other local therapies or supportive care alone were excluded. We analyzed survival with Cox proportional hazard modeling.</p><p><strong>Results: </strong>We identified 61 patients who received L-RT and 220 who received chemotherapy alone. At median follow-up of 11 months after diagnosis, median OS was 9 months (95% confidence interval [CI] 8-11) and 21 months (CI: 17-26) for patients receiving chemotherapy alone and L-RT, respectively. TRLF was the cause of death more often in the patients who received chemotherapy alone compared to those who received L-RT (82% vs. 47%; <i>p</i> = 0.001). On multivariable propensity score-matched analysis, associations with lower risk of death included duration of upfront chemotherapy (hazard ratio [HR] 0.82; <i>p</i> = 0.005) and receipt of L-RT (HR: 0.40; <i>p</i> = 0.002). The median OS from diagnosis for NCDB chemotherapy alone cohort was shorter than that of the institutional L-RT cohort (9 vs. 22 months; <i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>For M1 ICC, L-RT associated with a lower rate of death due to TRLF and longer OS versus those treated with chemotherapy alone. Prospective studies of L-RT in this setting are warranted.</p>","PeriodicalId":18156,"journal":{"name":"Liver Cancer","volume":"12 3","pages":"198-208"},"PeriodicalIF":10.5000,"publicationDate":"2023-03-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/2f/lic-2023-0012-0003-530134.PMC10427952.pdf","citationCount":"0","resultStr":"{\"title\":\"Definitive Liver Radiotherapy for Intrahepatic Cholangiocarcinoma with Extrahepatic Metastases.\",\"authors\":\"Brian De, Rituraj Upadhyay, Kaiping Liao, Tiffany Kumala, Christopher Shi, Grace Dodoo, Joseph Abi Jaoude, Kelsey L Corrigan, Gohar S Manzar, Kathryn E Marqueen, Vincent Bernard, Sunyoung S Lee, Kanwal P S Raghav, Jean-Nicolas Vauthey, Ching-Wei D Tzeng, Hop S Tran Cao, Grace Lee, Jennifer Y Wo, Theodore S Hong, Christopher H Crane, Bruce D Minsky, Grace L Smith, Emma B Holliday, Cullen M Taniguchi, Albert C Koong, Prajnan Das, Milind Javle, Ethan B Ludmir, Eugene J Koay\",\"doi\":\"10.1159/000530134\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Tumor-related liver failure (TRLF) is the most common cause of death in patients with intrahepatic cholangiocarcinoma (ICC). Though we previously showed that liver radiotherapy (L-RT) for locally advanced ICC is associated with less frequent TRLF and longer overall survival (OS), the role of L-RT for patients with extrahepatic metastatic disease (M1) remains undefined. We sought to compare outcomes for M1 ICC patients treated with and without L-RT.</p><p><strong>Methods: </strong>We reviewed ICC patients that found to have M1 disease at initial diagnosis at a single institution between 2010 and 2021 who received L-RT, matching them with an institutional cohort by propensity score and a National Cancer Database (NCDB) cohort by frequency technique. The median biologically effective dose was 97.5 Gy (interquartile range 80.5-97.9 Gy) for L-RT. Patients treated with other local therapies or supportive care alone were excluded. We analyzed survival with Cox proportional hazard modeling.</p><p><strong>Results: </strong>We identified 61 patients who received L-RT and 220 who received chemotherapy alone. At median follow-up of 11 months after diagnosis, median OS was 9 months (95% confidence interval [CI] 8-11) and 21 months (CI: 17-26) for patients receiving chemotherapy alone and L-RT, respectively. TRLF was the cause of death more often in the patients who received chemotherapy alone compared to those who received L-RT (82% vs. 47%; <i>p</i> = 0.001). On multivariable propensity score-matched analysis, associations with lower risk of death included duration of upfront chemotherapy (hazard ratio [HR] 0.82; <i>p</i> = 0.005) and receipt of L-RT (HR: 0.40; <i>p</i> = 0.002). The median OS from diagnosis for NCDB chemotherapy alone cohort was shorter than that of the institutional L-RT cohort (9 vs. 22 months; <i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>For M1 ICC, L-RT associated with a lower rate of death due to TRLF and longer OS versus those treated with chemotherapy alone. Prospective studies of L-RT in this setting are warranted.</p>\",\"PeriodicalId\":18156,\"journal\":{\"name\":\"Liver Cancer\",\"volume\":\"12 3\",\"pages\":\"198-208\"},\"PeriodicalIF\":10.5000,\"publicationDate\":\"2023-03-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/2f/lic-2023-0012-0003-530134.PMC10427952.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Liver Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000530134\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Liver Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000530134","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Definitive Liver Radiotherapy for Intrahepatic Cholangiocarcinoma with Extrahepatic Metastases.
Introduction: Tumor-related liver failure (TRLF) is the most common cause of death in patients with intrahepatic cholangiocarcinoma (ICC). Though we previously showed that liver radiotherapy (L-RT) for locally advanced ICC is associated with less frequent TRLF and longer overall survival (OS), the role of L-RT for patients with extrahepatic metastatic disease (M1) remains undefined. We sought to compare outcomes for M1 ICC patients treated with and without L-RT.
Methods: We reviewed ICC patients that found to have M1 disease at initial diagnosis at a single institution between 2010 and 2021 who received L-RT, matching them with an institutional cohort by propensity score and a National Cancer Database (NCDB) cohort by frequency technique. The median biologically effective dose was 97.5 Gy (interquartile range 80.5-97.9 Gy) for L-RT. Patients treated with other local therapies or supportive care alone were excluded. We analyzed survival with Cox proportional hazard modeling.
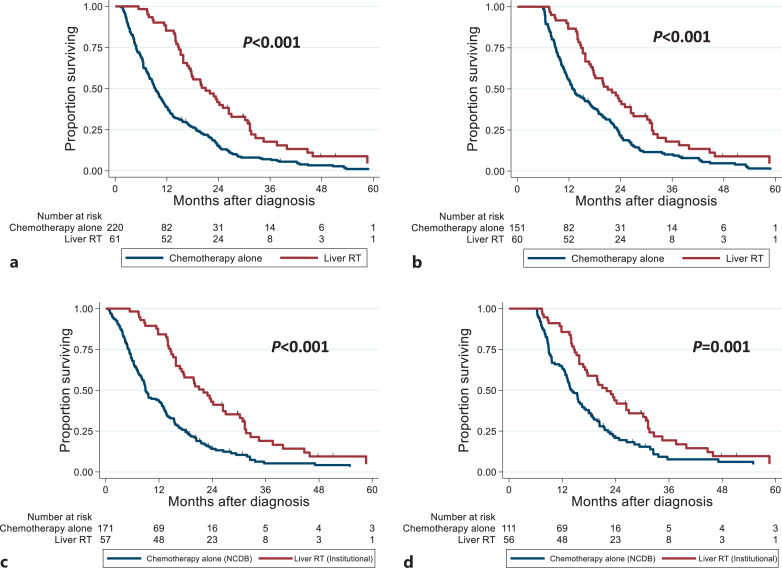
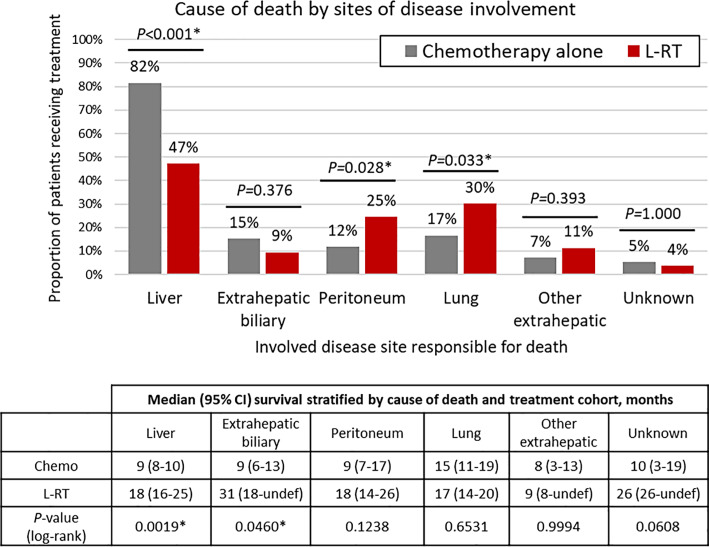
Results: We identified 61 patients who received L-RT and 220 who received chemotherapy alone. At median follow-up of 11 months after diagnosis, median OS was 9 months (95% confidence interval [CI] 8-11) and 21 months (CI: 17-26) for patients receiving chemotherapy alone and L-RT, respectively. TRLF was the cause of death more often in the patients who received chemotherapy alone compared to those who received L-RT (82% vs. 47%; p = 0.001). On multivariable propensity score-matched analysis, associations with lower risk of death included duration of upfront chemotherapy (hazard ratio [HR] 0.82; p = 0.005) and receipt of L-RT (HR: 0.40; p = 0.002). The median OS from diagnosis for NCDB chemotherapy alone cohort was shorter than that of the institutional L-RT cohort (9 vs. 22 months; p < 0.001).
Conclusion: For M1 ICC, L-RT associated with a lower rate of death due to TRLF and longer OS versus those treated with chemotherapy alone. Prospective studies of L-RT in this setting are warranted.
期刊介绍:
Liver Cancer is a journal that serves the international community of researchers and clinicians by providing a platform for research results related to the causes, mechanisms, and therapy of liver cancer. It focuses on molecular carcinogenesis, prevention, surveillance, diagnosis, and treatment, including molecular targeted therapy. The journal publishes clinical and translational research in the field of liver cancer in both humans and experimental models. It publishes original and review articles and has an Impact Factor of 13.8. The journal is indexed and abstracted in various platforms including PubMed, PubMed Central, Web of Science, Science Citation Index, Science Citation Index Expanded, Google Scholar, DOAJ, Chemical Abstracts Service, Scopus, Embase, Pathway Studio, and WorldCat.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
