Saleem M Halablab, Ayman Alrazim, Christian Sadaka, Hasan Slika, Nour Adra, Wissam Ghusn, Manar Shmais, Ala I Sharara
{"title":"吸烟不是克罗恩病患者接受生物治疗手术的独立危险因素。","authors":"Saleem M Halablab, Ayman Alrazim, Christian Sadaka, Hasan Slika, Nour Adra, Wissam Ghusn, Manar Shmais, Ala I Sharara","doi":"10.1159/000530689","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The development and course of inflammatory bowel disease appear to be influenced by environmental factors. Particularly, smoking has been shown to assume a harmful role in Crohn's disease (CD) and a protective role in ulcerative colitis. This study aims to examine the effect of smoking on need for surgery in patients with moderate to severe CD receiving biologic therapy.</p><p><strong>Methods: </strong>This was a retrospective study of adult patients with CD at a University Medical Center over a 20-year period.</p><p><strong>Results: </strong>A total of 251 patients were included (mean age 36.0 ± 15.0; 70.1% males; current, former, and nonsmokers: 44.2%, 11.6%, and 43.8%, respectively). Mean duration on biologics was 5.0 ± 3.1 years (>2/3 received anti-TNFs, followed by ustekinumab in 25.9%) and a third of patients (29.5%) received more than one biologic. Disease-related surgeries (abdominal, perianal, or both) occurred in 97 patients (38.6%): 50 patients had surgeries prior to starting biologics only, 41 had some surgeries after, and 6 had insufficient information. There was no significant difference in surgeries between ever-smokers (current or previous) versus nonsmokers in the overall study group. On logistic regression, the odds of having any CD surgery were higher in patients with longer disease duration (OR = 1.05, 95% CI = 1.01, 1.09) and in those receiving more than one biologic (OR = 2.31, 95% CI = 1.16, 4.59). However, among patients who had surgery prior to biologic therapy, smokers were more likely to have perianal surgery compared to nonsmokers (OR = 10.6, 95% CI = 2.0, 57.4; <i>p</i> = 0.006).</p><p><strong>Conclusion: </strong>In biologic-naive CD patients requiring surgery, smoking is an independent predictor of perianal surgery. Smoking, however, is not an independent risk factor for surgery in this cohort after starting biologics. The risk of surgery in those patients is primarily associated with disease duration and the use of more than one biologic.</p>","PeriodicalId":13605,"journal":{"name":"Inflammatory Intestinal Diseases","volume":"8 1","pages":"34-40"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10315011/pdf/","citationCount":"0","resultStr":"{\"title\":\"Smoking Is Not an Independent Risk Factor for Surgery in Patients with Crohn's Disease on Biologic Therapy.\",\"authors\":\"Saleem M Halablab, Ayman Alrazim, Christian Sadaka, Hasan Slika, Nour Adra, Wissam Ghusn, Manar Shmais, Ala I Sharara\",\"doi\":\"10.1159/000530689\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The development and course of inflammatory bowel disease appear to be influenced by environmental factors. Particularly, smoking has been shown to assume a harmful role in Crohn's disease (CD) and a protective role in ulcerative colitis. This study aims to examine the effect of smoking on need for surgery in patients with moderate to severe CD receiving biologic therapy.</p><p><strong>Methods: </strong>This was a retrospective study of adult patients with CD at a University Medical Center over a 20-year period.</p><p><strong>Results: </strong>A total of 251 patients were included (mean age 36.0 ± 15.0; 70.1% males; current, former, and nonsmokers: 44.2%, 11.6%, and 43.8%, respectively). Mean duration on biologics was 5.0 ± 3.1 years (>2/3 received anti-TNFs, followed by ustekinumab in 25.9%) and a third of patients (29.5%) received more than one biologic. Disease-related surgeries (abdominal, perianal, or both) occurred in 97 patients (38.6%): 50 patients had surgeries prior to starting biologics only, 41 had some surgeries after, and 6 had insufficient information. There was no significant difference in surgeries between ever-smokers (current or previous) versus nonsmokers in the overall study group. On logistic regression, the odds of having any CD surgery were higher in patients with longer disease duration (OR = 1.05, 95% CI = 1.01, 1.09) and in those receiving more than one biologic (OR = 2.31, 95% CI = 1.16, 4.59). However, among patients who had surgery prior to biologic therapy, smokers were more likely to have perianal surgery compared to nonsmokers (OR = 10.6, 95% CI = 2.0, 57.4; <i>p</i> = 0.006).</p><p><strong>Conclusion: </strong>In biologic-naive CD patients requiring surgery, smoking is an independent predictor of perianal surgery. Smoking, however, is not an independent risk factor for surgery in this cohort after starting biologics. The risk of surgery in those patients is primarily associated with disease duration and the use of more than one biologic.</p>\",\"PeriodicalId\":13605,\"journal\":{\"name\":\"Inflammatory Intestinal Diseases\",\"volume\":\"8 1\",\"pages\":\"34-40\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10315011/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Inflammatory Intestinal Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000530689\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Inflammatory Intestinal Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000530689","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
炎症性肠病的发展和病程似乎受环境因素的影响。特别是,吸烟已被证明在克罗恩病(CD)中起有害作用,在溃疡性结肠炎中起保护作用。本研究旨在探讨吸烟对接受生物治疗的中重度CD患者手术需求的影响。方法:这是一项对大学医学中心20年期间的成年乳糜泻患者的回顾性研究。结果:共纳入251例患者(平均年龄36.0±15.0;男性70.1%;目前、曾经和不吸烟者:分别为44.2%、11.6%和43.8%)。生物制剂的平均持续时间为5.0±3.1年(>2/3接受了抗tnf,其次是25.9%的ustekinumab),三分之一的患者(29.5%)接受了一种以上的生物制剂。97例患者(38.6%)进行了与疾病相关的手术(腹部、肛周或两者):50例患者仅在开始使用生物制剂前进行了手术,41例患者在开始使用生物制剂后进行了一些手术,6例患者信息不足。在整个研究组中,吸烟者(现在或以前)与不吸烟者之间的手术没有显著差异。在logistic回归中,病程较长的患者(OR = 1.05, 95% CI = 1.01, 1.09)和接受一种以上生物制剂治疗的患者(OR = 2.31, 95% CI = 1.16, 4.59)接受任何CD手术的几率更高。然而,在生物治疗前进行手术的患者中,吸烟者比不吸烟者更有可能进行肛周手术(OR = 10.6, 95% CI = 2.0, 57.4;P = 0.006)。结论:在需要手术的生物源性乳糜泻患者中,吸烟是肛周手术的独立预测因素。然而,在该队列中,吸烟并不是开始使用生物制剂后手术的独立危险因素。这些患者的手术风险主要与病程和使用一种以上生物制剂有关。
Smoking Is Not an Independent Risk Factor for Surgery in Patients with Crohn's Disease on Biologic Therapy.
Introduction: The development and course of inflammatory bowel disease appear to be influenced by environmental factors. Particularly, smoking has been shown to assume a harmful role in Crohn's disease (CD) and a protective role in ulcerative colitis. This study aims to examine the effect of smoking on need for surgery in patients with moderate to severe CD receiving biologic therapy.
Methods: This was a retrospective study of adult patients with CD at a University Medical Center over a 20-year period.
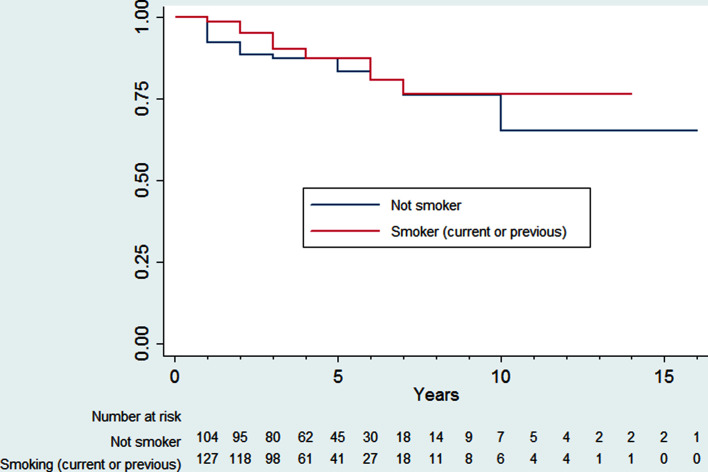
Results: A total of 251 patients were included (mean age 36.0 ± 15.0; 70.1% males; current, former, and nonsmokers: 44.2%, 11.6%, and 43.8%, respectively). Mean duration on biologics was 5.0 ± 3.1 years (>2/3 received anti-TNFs, followed by ustekinumab in 25.9%) and a third of patients (29.5%) received more than one biologic. Disease-related surgeries (abdominal, perianal, or both) occurred in 97 patients (38.6%): 50 patients had surgeries prior to starting biologics only, 41 had some surgeries after, and 6 had insufficient information. There was no significant difference in surgeries between ever-smokers (current or previous) versus nonsmokers in the overall study group. On logistic regression, the odds of having any CD surgery were higher in patients with longer disease duration (OR = 1.05, 95% CI = 1.01, 1.09) and in those receiving more than one biologic (OR = 2.31, 95% CI = 1.16, 4.59). However, among patients who had surgery prior to biologic therapy, smokers were more likely to have perianal surgery compared to nonsmokers (OR = 10.6, 95% CI = 2.0, 57.4; p = 0.006).
Conclusion: In biologic-naive CD patients requiring surgery, smoking is an independent predictor of perianal surgery. Smoking, however, is not an independent risk factor for surgery in this cohort after starting biologics. The risk of surgery in those patients is primarily associated with disease duration and the use of more than one biologic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
