Kavita Singh, Awantika Joshi, Nikhil Srinivasapura Venkateshmurthy, Rahul Rahul, Mark D Huffman, Nikhil Tandon, Dorairaj Prabhakaran
{"title":"印度心血管疾病护理循证策略优先级的德尔菲研究。","authors":"Kavita Singh, Awantika Joshi, Nikhil Srinivasapura Venkateshmurthy, Rahul Rahul, Mark D Huffman, Nikhil Tandon, Dorairaj Prabhakaran","doi":"10.1007/s43477-023-00087-2","DOIUrl":null,"url":null,"abstract":"<p><p>Providing quality cardiovascular disease (CVD) care in low resource setting requires understanding of priority and effective interventions. This study aimed to identify and prioritize evidence-based quality improvement strategies for CVD care in India using a modified two-round Delphi process in which, we asked 46 experts (clinicians, researchers, program implementers and policy makers) to rate 25 proven CVD care strategies grouped into: (1) patient support, (2) information communication technology (ICT) for health, (3) group problem solving, (4) training, and (5) multicomponent strategy on a scale of 1 (highest/best)-5 (lowest/worst) on priority, relative advantage, and feasibility. Subsequently, we convened an expert consensus panel of 32 members to deliberate and achieve consensus regarding the prioritized set of strategies for CVD care. The Delphi study found that group problem solving strategies achieved the best score for priority (1.80) but fared poorly on feasibility (2.88). Compared to others, multicomponent strategies were rated favorably across all domains (priority = 1.84, relative advantage = 1.94, and feasibility = 2.40). The ICT for health strategies achieved the worst scores for priority = 2.01, relative advantage = 2.31, and feasibility = 2.85. Training and patient support strategies scored moderately across all domains. The expert panel narrowed the selection of a multicomponent strategy consisting of (1) electronic health records with clinical decision-support system, (2) non-physician health worker facilitated care, (3) patient education materials, (4) text-message based reminders for healthy lifestyle, and (5) audit and feedback report for providers. Future research will evaluate the real-world feasibility and effectiveness of the multicomponent strategy in patients with CVD in a low- and middle-income country setting.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s43477-023-00087-2.</p>","PeriodicalId":73165,"journal":{"name":"Global implementation research and applications","volume":" ","pages":"1-12"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10240122/pdf/","citationCount":"1","resultStr":"{\"title\":\"A Delphi Study to Prioritize Evidence-Based Strategies for Cardiovascular Disease Care in India.\",\"authors\":\"Kavita Singh, Awantika Joshi, Nikhil Srinivasapura Venkateshmurthy, Rahul Rahul, Mark D Huffman, Nikhil Tandon, Dorairaj Prabhakaran\",\"doi\":\"10.1007/s43477-023-00087-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Providing quality cardiovascular disease (CVD) care in low resource setting requires understanding of priority and effective interventions. This study aimed to identify and prioritize evidence-based quality improvement strategies for CVD care in India using a modified two-round Delphi process in which, we asked 46 experts (clinicians, researchers, program implementers and policy makers) to rate 25 proven CVD care strategies grouped into: (1) patient support, (2) information communication technology (ICT) for health, (3) group problem solving, (4) training, and (5) multicomponent strategy on a scale of 1 (highest/best)-5 (lowest/worst) on priority, relative advantage, and feasibility. Subsequently, we convened an expert consensus panel of 32 members to deliberate and achieve consensus regarding the prioritized set of strategies for CVD care. The Delphi study found that group problem solving strategies achieved the best score for priority (1.80) but fared poorly on feasibility (2.88). Compared to others, multicomponent strategies were rated favorably across all domains (priority = 1.84, relative advantage = 1.94, and feasibility = 2.40). The ICT for health strategies achieved the worst scores for priority = 2.01, relative advantage = 2.31, and feasibility = 2.85. Training and patient support strategies scored moderately across all domains. The expert panel narrowed the selection of a multicomponent strategy consisting of (1) electronic health records with clinical decision-support system, (2) non-physician health worker facilitated care, (3) patient education materials, (4) text-message based reminders for healthy lifestyle, and (5) audit and feedback report for providers. Future research will evaluate the real-world feasibility and effectiveness of the multicomponent strategy in patients with CVD in a low- and middle-income country setting.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s43477-023-00087-2.</p>\",\"PeriodicalId\":73165,\"journal\":{\"name\":\"Global implementation research and applications\",\"volume\":\" \",\"pages\":\"1-12\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10240122/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global implementation research and applications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s43477-023-00087-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global implementation research and applications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43477-023-00087-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Delphi Study to Prioritize Evidence-Based Strategies for Cardiovascular Disease Care in India.
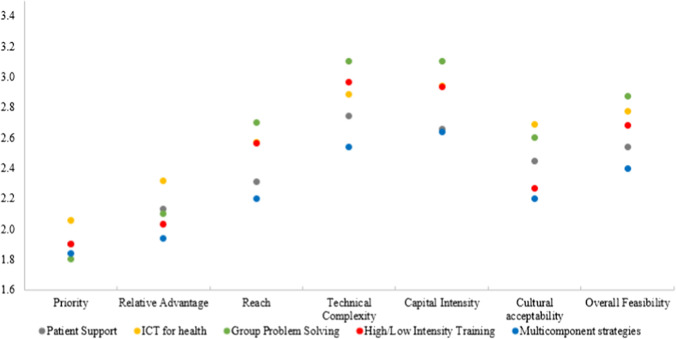
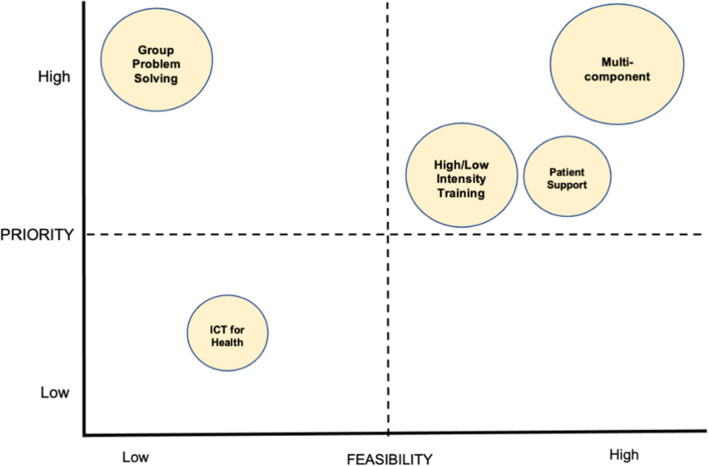
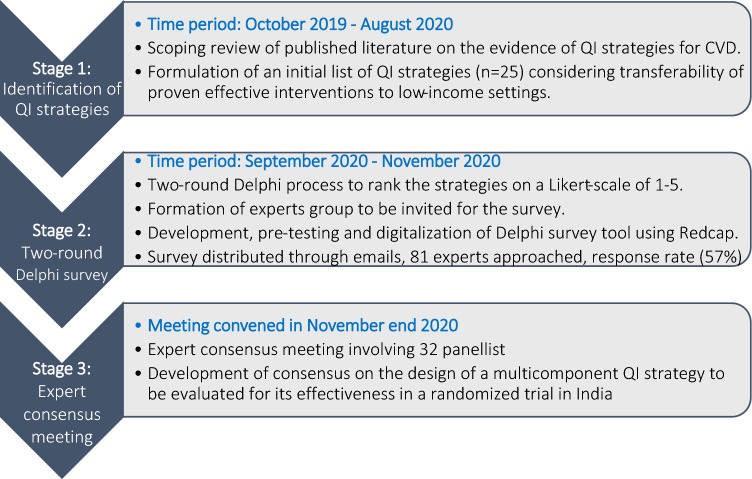
Providing quality cardiovascular disease (CVD) care in low resource setting requires understanding of priority and effective interventions. This study aimed to identify and prioritize evidence-based quality improvement strategies for CVD care in India using a modified two-round Delphi process in which, we asked 46 experts (clinicians, researchers, program implementers and policy makers) to rate 25 proven CVD care strategies grouped into: (1) patient support, (2) information communication technology (ICT) for health, (3) group problem solving, (4) training, and (5) multicomponent strategy on a scale of 1 (highest/best)-5 (lowest/worst) on priority, relative advantage, and feasibility. Subsequently, we convened an expert consensus panel of 32 members to deliberate and achieve consensus regarding the prioritized set of strategies for CVD care. The Delphi study found that group problem solving strategies achieved the best score for priority (1.80) but fared poorly on feasibility (2.88). Compared to others, multicomponent strategies were rated favorably across all domains (priority = 1.84, relative advantage = 1.94, and feasibility = 2.40). The ICT for health strategies achieved the worst scores for priority = 2.01, relative advantage = 2.31, and feasibility = 2.85. Training and patient support strategies scored moderately across all domains. The expert panel narrowed the selection of a multicomponent strategy consisting of (1) electronic health records with clinical decision-support system, (2) non-physician health worker facilitated care, (3) patient education materials, (4) text-message based reminders for healthy lifestyle, and (5) audit and feedback report for providers. Future research will evaluate the real-world feasibility and effectiveness of the multicomponent strategy in patients with CVD in a low- and middle-income country setting.
Supplementary information: The online version contains supplementary material available at 10.1007/s43477-023-00087-2.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
