Santhiya Iswarya Vinothini Udayakumar, Dohyoung Kim, So-Young Choi, Tae-Geon Kwon
{"title":"下颌不对称矢状支劈开截骨中骨间干扰的三维模拟。","authors":"Santhiya Iswarya Vinothini Udayakumar, Dohyoung Kim, So-Young Choi, Tae-Geon Kwon","doi":"10.1186/s40902-023-00400-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of this study was to evaluate the pattern of predicted interosseous interference and to determine the influencing factor to volume of bony interference using a computer-assisted simulation system. This retrospective study recruited 116 patients with mandibular prognathism who had undergone sagittal split ramus osteotomy (SSRO) with or without maxillary osteotomy. The patients were divided into 3 groups according to the amount of menton (Me) deviation: less than 2 mm (Group 1), 2-4 mm (Group 2), and more than 4 mm (Group 3). Changes in the distal segments following BSSRO and the volume of the interosseous interference between the proximal and distal segments were simulated after matching preoperative occlusion and postoperative expected occlusion with the cone-beam computed tomography data. Ramal inclinations and other skeletal measurements were analyzed before surgery, immediately after surgery, and at least 6 months after surgery.</p><p><strong>Results: </strong>The anticipated interosseous interference was more frequently noted on the contralateral side of chin deviation (long side) than the deviated site (short side) in Groups 2 and 3. More interference volume was predicted at the long side (186 ± 343.9 mm<sup>3</sup>) rather than the short side (54.4 ± 124.4 mm<sup>3</sup>) in Group 3 (p = 0.033). The bilateral difference in the volume of the interosseous interference of the osteotomized mandible was significantly correlated with the Me deviation (r = - 0.257, p = 0.009) and bilateral ramal inclination (r = 0.361, p < 0.001). The predictor variable that affected the volume of the osseous interference at each side was the amount of Me deviation (p = 0.010).</p><p><strong>Conclusion: </strong>By using the 3D simulation system, the potential site of bony collision could be visualized and successfully reduced intraoperatively. Since the osseous interference can be existed on any side, unilaterally or bilaterally, 3D surgical simulation is necessary before surgery to predict the osseous interference and improve the ramal inclination.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"45 1","pages":"32"},"PeriodicalIF":2.8000,"publicationDate":"2023-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10505600/pdf/","citationCount":"0","resultStr":"{\"title\":\"3D simulation of interosseous interference in sagittal split ramus osteotomy for mandibular asymmetry.\",\"authors\":\"Santhiya Iswarya Vinothini Udayakumar, Dohyoung Kim, So-Young Choi, Tae-Geon Kwon\",\"doi\":\"10.1186/s40902-023-00400-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The purpose of this study was to evaluate the pattern of predicted interosseous interference and to determine the influencing factor to volume of bony interference using a computer-assisted simulation system. This retrospective study recruited 116 patients with mandibular prognathism who had undergone sagittal split ramus osteotomy (SSRO) with or without maxillary osteotomy. The patients were divided into 3 groups according to the amount of menton (Me) deviation: less than 2 mm (Group 1), 2-4 mm (Group 2), and more than 4 mm (Group 3). Changes in the distal segments following BSSRO and the volume of the interosseous interference between the proximal and distal segments were simulated after matching preoperative occlusion and postoperative expected occlusion with the cone-beam computed tomography data. Ramal inclinations and other skeletal measurements were analyzed before surgery, immediately after surgery, and at least 6 months after surgery.</p><p><strong>Results: </strong>The anticipated interosseous interference was more frequently noted on the contralateral side of chin deviation (long side) than the deviated site (short side) in Groups 2 and 3. More interference volume was predicted at the long side (186 ± 343.9 mm<sup>3</sup>) rather than the short side (54.4 ± 124.4 mm<sup>3</sup>) in Group 3 (p = 0.033). The bilateral difference in the volume of the interosseous interference of the osteotomized mandible was significantly correlated with the Me deviation (r = - 0.257, p = 0.009) and bilateral ramal inclination (r = 0.361, p < 0.001). The predictor variable that affected the volume of the osseous interference at each side was the amount of Me deviation (p = 0.010).</p><p><strong>Conclusion: </strong>By using the 3D simulation system, the potential site of bony collision could be visualized and successfully reduced intraoperatively. Since the osseous interference can be existed on any side, unilaterally or bilaterally, 3D surgical simulation is necessary before surgery to predict the osseous interference and improve the ramal inclination.</p>\",\"PeriodicalId\":18357,\"journal\":{\"name\":\"Maxillofacial Plastic and Reconstructive Surgery\",\"volume\":\"45 1\",\"pages\":\"32\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10505600/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Maxillofacial Plastic and Reconstructive Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40902-023-00400-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-023-00400-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
3D simulation of interosseous interference in sagittal split ramus osteotomy for mandibular asymmetry.
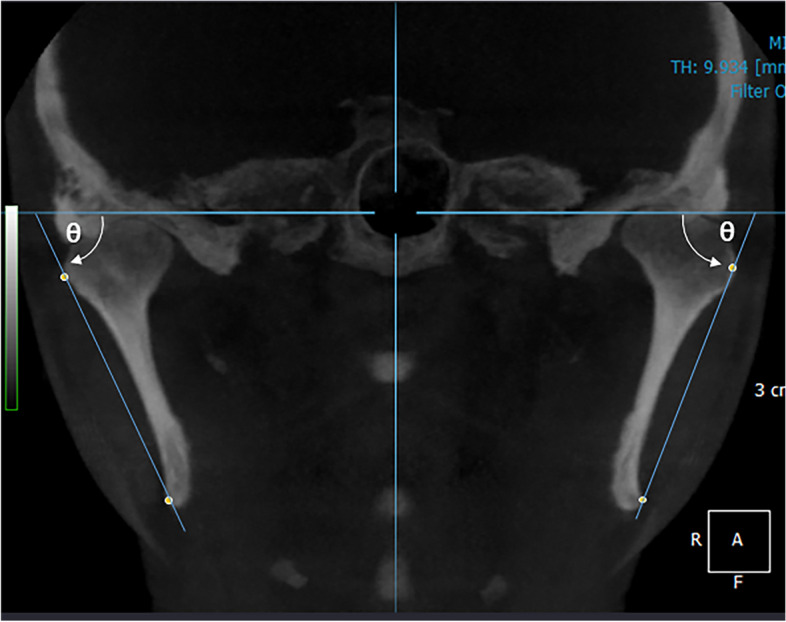
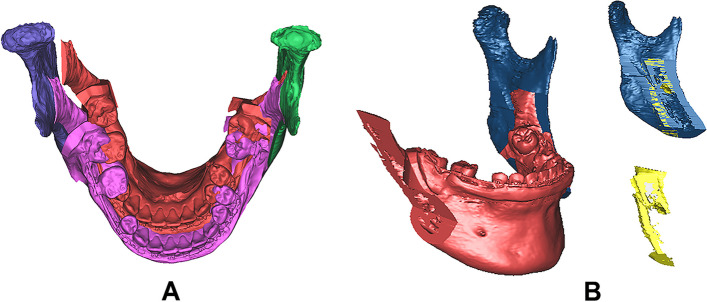
Background: The purpose of this study was to evaluate the pattern of predicted interosseous interference and to determine the influencing factor to volume of bony interference using a computer-assisted simulation system. This retrospective study recruited 116 patients with mandibular prognathism who had undergone sagittal split ramus osteotomy (SSRO) with or without maxillary osteotomy. The patients were divided into 3 groups according to the amount of menton (Me) deviation: less than 2 mm (Group 1), 2-4 mm (Group 2), and more than 4 mm (Group 3). Changes in the distal segments following BSSRO and the volume of the interosseous interference between the proximal and distal segments were simulated after matching preoperative occlusion and postoperative expected occlusion with the cone-beam computed tomography data. Ramal inclinations and other skeletal measurements were analyzed before surgery, immediately after surgery, and at least 6 months after surgery.
Results: The anticipated interosseous interference was more frequently noted on the contralateral side of chin deviation (long side) than the deviated site (short side) in Groups 2 and 3. More interference volume was predicted at the long side (186 ± 343.9 mm3) rather than the short side (54.4 ± 124.4 mm3) in Group 3 (p = 0.033). The bilateral difference in the volume of the interosseous interference of the osteotomized mandible was significantly correlated with the Me deviation (r = - 0.257, p = 0.009) and bilateral ramal inclination (r = 0.361, p < 0.001). The predictor variable that affected the volume of the osseous interference at each side was the amount of Me deviation (p = 0.010).
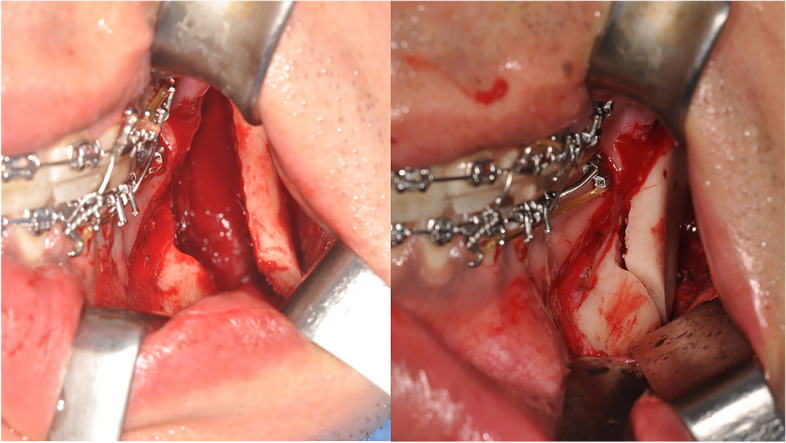
Conclusion: By using the 3D simulation system, the potential site of bony collision could be visualized and successfully reduced intraoperatively. Since the osseous interference can be existed on any side, unilaterally or bilaterally, 3D surgical simulation is necessary before surgery to predict the osseous interference and improve the ramal inclination.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
