Mariana L Matos, Maria Inês T S Matos, Carlos M S P M Grijó, Marta F S Patacho, António J S Almeida
{"title":"梅-瑟纳综合征1例报告。","authors":"Mariana L Matos, Maria Inês T S Matos, Carlos M S P M Grijó, Marta F S Patacho, António J S Almeida","doi":"10.1097/j.pbj.0000000000000224","DOIUrl":null,"url":null,"abstract":"May-Thurner syndrome (MTS) was first described in 1957 as a rare vascular condition in which chronic pulsations of the right common iliac artery (RCIA), which overlies the left common iliac vein (LCIV), lead to spur formation along the wall of this vein. This anatomic condition is not uncommon in healthy individuals, according to both autopsies and imaging studies in asymptomatic populations, and affects most commonly women in their third to fifth decade of life. Some patients will have symptoms of chronic venous disease (CVD) with extremity pain, swelling, and varicose vein ulcerations. However, the prevalence of associated deep vein thrombosis (DVT) is relatively rare (2%–3%), suggesting that the presence of this anatomic finding alone may not increase the risk of DVT. In situations with hypercoagulable status, endothelial injury, and venous stasis (present in this condition), there is increased risk to DVT, as postulated in the Virchow Triad. Although there are no standardized diagnostic criteria, imaging has an important role in identifying this condition in patients with signs and symptoms of MTS. Because of its noninvasive character, ultrasound is frequently the first chosen modality in patients with DVT. However, visualization of common iliac vein segments is technically challenging, and ultrasound may miss the diagnosis of MTS. Although the gold standard for the diagnosis of MTS is conventional venography with intravenous ultrasound (IVUS), the most common and useful imaging scan is computed tomography (CT) scan because of its sensitivity and availability. Invasive catheter-based strategies have gained interest because of high association of MTS and iliofemoral thrombosis with postthrombotic syndrome (PTS). Endovascular stent may be performed acutely after initial catheter-directed thrombolysis or in chronic symptomatic patients, namely after PTS development. This case illustrates this condition as well as its challenging diagnosis and treatment. We report a 19-year-old woman, presenting in the emergency room (ER) with dyspnea, pleuritic chest pain, fever, and mushy stools, lasting for two weeks. The patient had no relevant medical history and was only medicated with oral anticonception. The clinical examination at the ER revealed a hemodynamically stable patient, with a slight tachycardia of 110 bpm. The remaining physical examination was unremarkable. The electrocardiogram showed a sinus rhythm, with no abnormalities. The chest X-ray presented a normal cardiothoracic index and no abnormal mass or consolidation. Laboratory study showed a microcytic anemia (10.6 g/dL [12.0–16.0g/dL]) and elevated C-reactive protein (182 mg/L [,3 mg/L]). Blood and urine cultures were obtained, and the patient was admitted to the Infectious Diseases ward because of initial suspicion of infectious colitis. The maintenance of tachycardia and pleuritic chest pain and the development of left lower limb enlargement and pain (not mentioned before) led to the performance of a thoracoabdominal-pelvic CT scan 5 days after admission. This examination showed signs of bilateral pulmonary embolism with segmental pulmonary infarction (Fig. 1) and thrombosis of the LCIV and its internal and external branches. An ultrasound was also performed and revealed DVT of the left ilio-femoralpopliteal vein. At this point, the patient started anticoagulation therapy with enoxaparin 1mg/kg/day and was transferred to the Internal Medicine ward. A multidisciplinary discussion with the Vascular Surgery team was proposed. After about two weeks, the case was discussed with the Vascular Surgery team, and the images were reviewed with the demonstration of LCIV external compression by RCIA, not mentioned previously in the CT scan report (Fig. 2). Given the time since the beginning of the symptoms, a conservative approach with oral anticoagulation was decided, and the patient was thereafter discharged and oriented to Internal Medicine and Vascular Surgery appointments. After 10 months of discharge, the CT scan was repeated and demonstrated repermeabilization of lower limb veins, maintaining a filling defect across LICV, suggesting residual thrombus. After 1-year follow-up, the patient developed PTS and was submitted to stenting of the LICV. The follow-up CT scan (three months after the procedure) showed a well-positioned and permeable stent from the femoral vein to the inferior vena cava (IVC) (Fig. 3). After the procedure, the symptoms resolved and the patient remained asymptomatic and was treated with oral anticoagulation for another 12 months. One year after stenting, no symptoms were reported, and a low-dose aspirin treatment was started, with oral anticoagulation withdrawal. Our case describes an underdiagnosed cause of DVT, presenting as a pulmonary embolism. This case illustrates the complications associated with this condition and the risk of delayed invasive treatment that may reduce the associated morbidity. PTS, characterized by diverse signs and symptoms of venous insufficiency, such as pain, swelling, paresthesia, skin hyperpigmentation, and, eventually, venous ulceration, is a frequent complication of DVT. It affects about 20%–60% of patients, Internal Medicine Department, Centro Hospitalar Universitário São João, Porto, Portugal","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"8 4","pages":"e224"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/84/pj9-8-e224.PMC10400067.pdf","citationCount":"0","resultStr":"{\"title\":\"May-Thurner syndrome: a case report.\",\"authors\":\"Mariana L Matos, Maria Inês T S Matos, Carlos M S P M Grijó, Marta F S Patacho, António J S Almeida\",\"doi\":\"10.1097/j.pbj.0000000000000224\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"May-Thurner syndrome (MTS) was first described in 1957 as a rare vascular condition in which chronic pulsations of the right common iliac artery (RCIA), which overlies the left common iliac vein (LCIV), lead to spur formation along the wall of this vein. This anatomic condition is not uncommon in healthy individuals, according to both autopsies and imaging studies in asymptomatic populations, and affects most commonly women in their third to fifth decade of life. Some patients will have symptoms of chronic venous disease (CVD) with extremity pain, swelling, and varicose vein ulcerations. However, the prevalence of associated deep vein thrombosis (DVT) is relatively rare (2%–3%), suggesting that the presence of this anatomic finding alone may not increase the risk of DVT. In situations with hypercoagulable status, endothelial injury, and venous stasis (present in this condition), there is increased risk to DVT, as postulated in the Virchow Triad. Although there are no standardized diagnostic criteria, imaging has an important role in identifying this condition in patients with signs and symptoms of MTS. Because of its noninvasive character, ultrasound is frequently the first chosen modality in patients with DVT. However, visualization of common iliac vein segments is technically challenging, and ultrasound may miss the diagnosis of MTS. Although the gold standard for the diagnosis of MTS is conventional venography with intravenous ultrasound (IVUS), the most common and useful imaging scan is computed tomography (CT) scan because of its sensitivity and availability. Invasive catheter-based strategies have gained interest because of high association of MTS and iliofemoral thrombosis with postthrombotic syndrome (PTS). Endovascular stent may be performed acutely after initial catheter-directed thrombolysis or in chronic symptomatic patients, namely after PTS development. This case illustrates this condition as well as its challenging diagnosis and treatment. We report a 19-year-old woman, presenting in the emergency room (ER) with dyspnea, pleuritic chest pain, fever, and mushy stools, lasting for two weeks. The patient had no relevant medical history and was only medicated with oral anticonception. The clinical examination at the ER revealed a hemodynamically stable patient, with a slight tachycardia of 110 bpm. The remaining physical examination was unremarkable. The electrocardiogram showed a sinus rhythm, with no abnormalities. The chest X-ray presented a normal cardiothoracic index and no abnormal mass or consolidation. Laboratory study showed a microcytic anemia (10.6 g/dL [12.0–16.0g/dL]) and elevated C-reactive protein (182 mg/L [,3 mg/L]). Blood and urine cultures were obtained, and the patient was admitted to the Infectious Diseases ward because of initial suspicion of infectious colitis. The maintenance of tachycardia and pleuritic chest pain and the development of left lower limb enlargement and pain (not mentioned before) led to the performance of a thoracoabdominal-pelvic CT scan 5 days after admission. This examination showed signs of bilateral pulmonary embolism with segmental pulmonary infarction (Fig. 1) and thrombosis of the LCIV and its internal and external branches. An ultrasound was also performed and revealed DVT of the left ilio-femoralpopliteal vein. At this point, the patient started anticoagulation therapy with enoxaparin 1mg/kg/day and was transferred to the Internal Medicine ward. A multidisciplinary discussion with the Vascular Surgery team was proposed. After about two weeks, the case was discussed with the Vascular Surgery team, and the images were reviewed with the demonstration of LCIV external compression by RCIA, not mentioned previously in the CT scan report (Fig. 2). Given the time since the beginning of the symptoms, a conservative approach with oral anticoagulation was decided, and the patient was thereafter discharged and oriented to Internal Medicine and Vascular Surgery appointments. After 10 months of discharge, the CT scan was repeated and demonstrated repermeabilization of lower limb veins, maintaining a filling defect across LICV, suggesting residual thrombus. After 1-year follow-up, the patient developed PTS and was submitted to stenting of the LICV. The follow-up CT scan (three months after the procedure) showed a well-positioned and permeable stent from the femoral vein to the inferior vena cava (IVC) (Fig. 3). After the procedure, the symptoms resolved and the patient remained asymptomatic and was treated with oral anticoagulation for another 12 months. One year after stenting, no symptoms were reported, and a low-dose aspirin treatment was started, with oral anticoagulation withdrawal. Our case describes an underdiagnosed cause of DVT, presenting as a pulmonary embolism. This case illustrates the complications associated with this condition and the risk of delayed invasive treatment that may reduce the associated morbidity. PTS, characterized by diverse signs and symptoms of venous insufficiency, such as pain, swelling, paresthesia, skin hyperpigmentation, and, eventually, venous ulceration, is a frequent complication of DVT. It affects about 20%–60% of patients, Internal Medicine Department, Centro Hospitalar Universitário São João, Porto, Portugal\",\"PeriodicalId\":74479,\"journal\":{\"name\":\"Porto biomedical journal\",\"volume\":\"8 4\",\"pages\":\"e224\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/84/pj9-8-e224.PMC10400067.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Porto biomedical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/j.pbj.0000000000000224\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000224","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
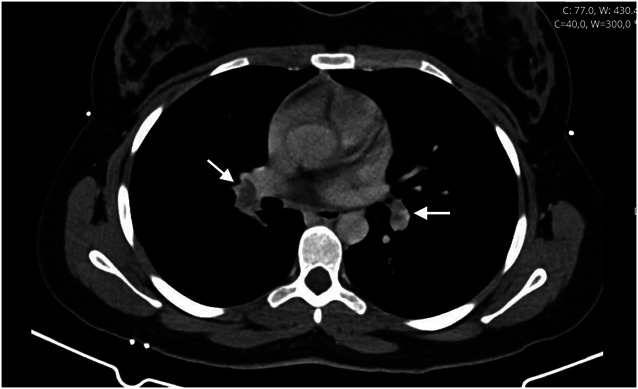
May-Thurner syndrome (MTS) was first described in 1957 as a rare vascular condition in which chronic pulsations of the right common iliac artery (RCIA), which overlies the left common iliac vein (LCIV), lead to spur formation along the wall of this vein. This anatomic condition is not uncommon in healthy individuals, according to both autopsies and imaging studies in asymptomatic populations, and affects most commonly women in their third to fifth decade of life. Some patients will have symptoms of chronic venous disease (CVD) with extremity pain, swelling, and varicose vein ulcerations. However, the prevalence of associated deep vein thrombosis (DVT) is relatively rare (2%–3%), suggesting that the presence of this anatomic finding alone may not increase the risk of DVT. In situations with hypercoagulable status, endothelial injury, and venous stasis (present in this condition), there is increased risk to DVT, as postulated in the Virchow Triad. Although there are no standardized diagnostic criteria, imaging has an important role in identifying this condition in patients with signs and symptoms of MTS. Because of its noninvasive character, ultrasound is frequently the first chosen modality in patients with DVT. However, visualization of common iliac vein segments is technically challenging, and ultrasound may miss the diagnosis of MTS. Although the gold standard for the diagnosis of MTS is conventional venography with intravenous ultrasound (IVUS), the most common and useful imaging scan is computed tomography (CT) scan because of its sensitivity and availability. Invasive catheter-based strategies have gained interest because of high association of MTS and iliofemoral thrombosis with postthrombotic syndrome (PTS). Endovascular stent may be performed acutely after initial catheter-directed thrombolysis or in chronic symptomatic patients, namely after PTS development. This case illustrates this condition as well as its challenging diagnosis and treatment. We report a 19-year-old woman, presenting in the emergency room (ER) with dyspnea, pleuritic chest pain, fever, and mushy stools, lasting for two weeks. The patient had no relevant medical history and was only medicated with oral anticonception. The clinical examination at the ER revealed a hemodynamically stable patient, with a slight tachycardia of 110 bpm. The remaining physical examination was unremarkable. The electrocardiogram showed a sinus rhythm, with no abnormalities. The chest X-ray presented a normal cardiothoracic index and no abnormal mass or consolidation. Laboratory study showed a microcytic anemia (10.6 g/dL [12.0–16.0g/dL]) and elevated C-reactive protein (182 mg/L [,3 mg/L]). Blood and urine cultures were obtained, and the patient was admitted to the Infectious Diseases ward because of initial suspicion of infectious colitis. The maintenance of tachycardia and pleuritic chest pain and the development of left lower limb enlargement and pain (not mentioned before) led to the performance of a thoracoabdominal-pelvic CT scan 5 days after admission. This examination showed signs of bilateral pulmonary embolism with segmental pulmonary infarction (Fig. 1) and thrombosis of the LCIV and its internal and external branches. An ultrasound was also performed and revealed DVT of the left ilio-femoralpopliteal vein. At this point, the patient started anticoagulation therapy with enoxaparin 1mg/kg/day and was transferred to the Internal Medicine ward. A multidisciplinary discussion with the Vascular Surgery team was proposed. After about two weeks, the case was discussed with the Vascular Surgery team, and the images were reviewed with the demonstration of LCIV external compression by RCIA, not mentioned previously in the CT scan report (Fig. 2). Given the time since the beginning of the symptoms, a conservative approach with oral anticoagulation was decided, and the patient was thereafter discharged and oriented to Internal Medicine and Vascular Surgery appointments. After 10 months of discharge, the CT scan was repeated and demonstrated repermeabilization of lower limb veins, maintaining a filling defect across LICV, suggesting residual thrombus. After 1-year follow-up, the patient developed PTS and was submitted to stenting of the LICV. The follow-up CT scan (three months after the procedure) showed a well-positioned and permeable stent from the femoral vein to the inferior vena cava (IVC) (Fig. 3). After the procedure, the symptoms resolved and the patient remained asymptomatic and was treated with oral anticoagulation for another 12 months. One year after stenting, no symptoms were reported, and a low-dose aspirin treatment was started, with oral anticoagulation withdrawal. Our case describes an underdiagnosed cause of DVT, presenting as a pulmonary embolism. This case illustrates the complications associated with this condition and the risk of delayed invasive treatment that may reduce the associated morbidity. PTS, characterized by diverse signs and symptoms of venous insufficiency, such as pain, swelling, paresthesia, skin hyperpigmentation, and, eventually, venous ulceration, is a frequent complication of DVT. It affects about 20%–60% of patients, Internal Medicine Department, Centro Hospitalar Universitário São João, Porto, Portugal





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
