{"title":"颈神经根病是心绞痛的隐性病因:颈源性心绞痛。","authors":"Eric Chun-Pu Chu","doi":"10.14740/jmc4025","DOIUrl":null,"url":null,"abstract":"<p><p>Patients presenting with chest pain to the emergency department constitute a diagnostic challenge as 77% of the patients' symptoms are not cardiac. Diagnostic uncertainty is a pervasive issue in primary care. A 56-year-old man presented with non-traumatic chest pain and chronic neck pain for 2 years, as well as numbness in his right third and fourth fingers for 6 months. It was not associated with palpitation, orthopnea or pedal edema. Except for hyperglycemia, no abnormal findings were found in diagnostic tests. At that time, he was being treated for type 2 diabetes using glucose-lowering drugs in order to lower his blood glucose and lessen his risk of heart disease. The cause of his chest pain remained unknown. Following a second opinion from an orthopedist, the patient was diagnosed with cervical radiculopathy and was treated with analgesics and physical therapy. Because the treatments had only provided temporary pain relief for the previous 6 months, he sought chiropractic care for pain relief. The patient's vital signs were stable and within normal limits during the assessment. A restricted neck movement, a positive Spurling test, and hypoesthesia in the right C7 dermatome were seen. Cervical radiographs revealed degenerative spondylosis with right C5/C6 neuroforaminal stenoses and bilateral C6/C7 neuroforaminal stenoses. A provisional diagnosis of cervical spondylotic radiculopathy associated with cervicogenic angina (CA) was made. Chiropractic procedures, including cervical manipulation, instrumented soft tissue mobilization, and motorized intermittent neck traction, were performed two to three times per week. After 3 months, the patient reported that the chest pain, neck pain, and radicular symptoms had completely resolved. Repeated radiographs taken during the 11th month follow-up revealed a comparable improvement in the increased spacing of the restricted neuroforamina, which could signify a beneficial alteration related to cervical function retrieval. CA is an angina-like chest pain caused by cervical spine disorders. This study adds to our understanding of the biomechanical impact of cervical radiculopathy on chest pain, which has largely been overlooked during diagnostic workups. Once cervical radiculopathy has been identified, CA symptoms can be eased by alleviating the noxious input stemming from the pinched nerve roots.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"13 11","pages":"545-550"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d1/05/jmc-13-545.PMC9728145.pdf","citationCount":"8","resultStr":"{\"title\":\"Cervical Radiculopathy as a Hidden Cause of Angina: Cervicogenic Angina.\",\"authors\":\"Eric Chun-Pu Chu\",\"doi\":\"10.14740/jmc4025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patients presenting with chest pain to the emergency department constitute a diagnostic challenge as 77% of the patients' symptoms are not cardiac. Diagnostic uncertainty is a pervasive issue in primary care. A 56-year-old man presented with non-traumatic chest pain and chronic neck pain for 2 years, as well as numbness in his right third and fourth fingers for 6 months. It was not associated with palpitation, orthopnea or pedal edema. Except for hyperglycemia, no abnormal findings were found in diagnostic tests. At that time, he was being treated for type 2 diabetes using glucose-lowering drugs in order to lower his blood glucose and lessen his risk of heart disease. The cause of his chest pain remained unknown. Following a second opinion from an orthopedist, the patient was diagnosed with cervical radiculopathy and was treated with analgesics and physical therapy. Because the treatments had only provided temporary pain relief for the previous 6 months, he sought chiropractic care for pain relief. The patient's vital signs were stable and within normal limits during the assessment. A restricted neck movement, a positive Spurling test, and hypoesthesia in the right C7 dermatome were seen. Cervical radiographs revealed degenerative spondylosis with right C5/C6 neuroforaminal stenoses and bilateral C6/C7 neuroforaminal stenoses. A provisional diagnosis of cervical spondylotic radiculopathy associated with cervicogenic angina (CA) was made. Chiropractic procedures, including cervical manipulation, instrumented soft tissue mobilization, and motorized intermittent neck traction, were performed two to three times per week. After 3 months, the patient reported that the chest pain, neck pain, and radicular symptoms had completely resolved. Repeated radiographs taken during the 11th month follow-up revealed a comparable improvement in the increased spacing of the restricted neuroforamina, which could signify a beneficial alteration related to cervical function retrieval. CA is an angina-like chest pain caused by cervical spine disorders. This study adds to our understanding of the biomechanical impact of cervical radiculopathy on chest pain, which has largely been overlooked during diagnostic workups. Once cervical radiculopathy has been identified, CA symptoms can be eased by alleviating the noxious input stemming from the pinched nerve roots.</p>\",\"PeriodicalId\":16279,\"journal\":{\"name\":\"Journal of Medical Cases\",\"volume\":\"13 11\",\"pages\":\"545-550\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d1/05/jmc-13-545.PMC9728145.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cervical Radiculopathy as a Hidden Cause of Angina: Cervicogenic Angina.
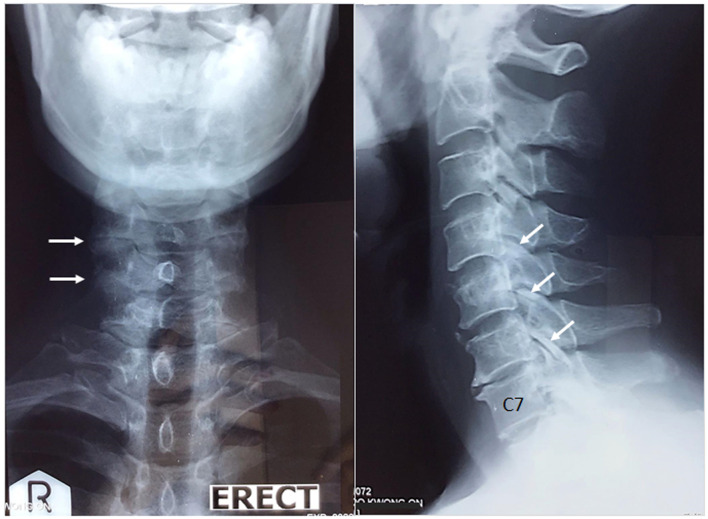
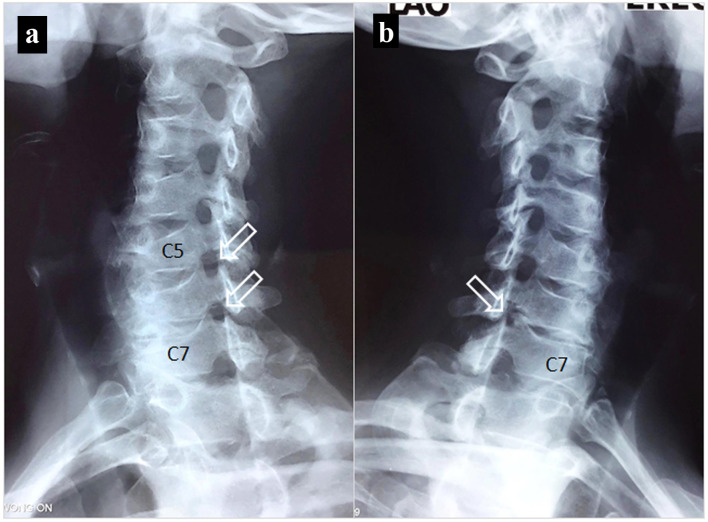
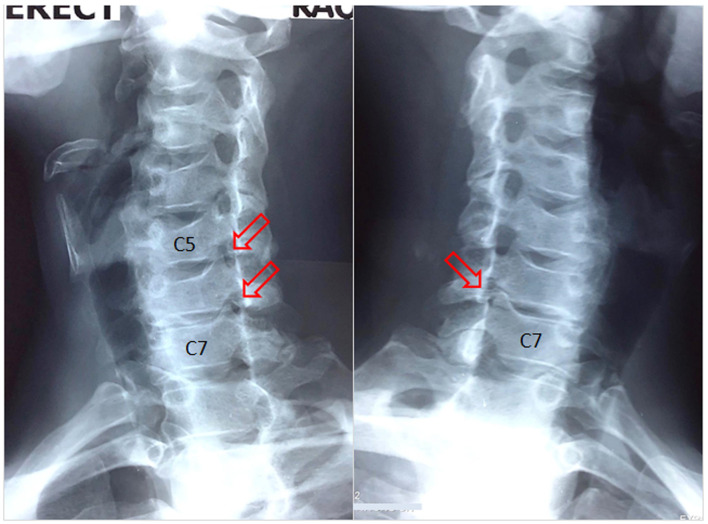
Patients presenting with chest pain to the emergency department constitute a diagnostic challenge as 77% of the patients' symptoms are not cardiac. Diagnostic uncertainty is a pervasive issue in primary care. A 56-year-old man presented with non-traumatic chest pain and chronic neck pain for 2 years, as well as numbness in his right third and fourth fingers for 6 months. It was not associated with palpitation, orthopnea or pedal edema. Except for hyperglycemia, no abnormal findings were found in diagnostic tests. At that time, he was being treated for type 2 diabetes using glucose-lowering drugs in order to lower his blood glucose and lessen his risk of heart disease. The cause of his chest pain remained unknown. Following a second opinion from an orthopedist, the patient was diagnosed with cervical radiculopathy and was treated with analgesics and physical therapy. Because the treatments had only provided temporary pain relief for the previous 6 months, he sought chiropractic care for pain relief. The patient's vital signs were stable and within normal limits during the assessment. A restricted neck movement, a positive Spurling test, and hypoesthesia in the right C7 dermatome were seen. Cervical radiographs revealed degenerative spondylosis with right C5/C6 neuroforaminal stenoses and bilateral C6/C7 neuroforaminal stenoses. A provisional diagnosis of cervical spondylotic radiculopathy associated with cervicogenic angina (CA) was made. Chiropractic procedures, including cervical manipulation, instrumented soft tissue mobilization, and motorized intermittent neck traction, were performed two to three times per week. After 3 months, the patient reported that the chest pain, neck pain, and radicular symptoms had completely resolved. Repeated radiographs taken during the 11th month follow-up revealed a comparable improvement in the increased spacing of the restricted neuroforamina, which could signify a beneficial alteration related to cervical function retrieval. CA is an angina-like chest pain caused by cervical spine disorders. This study adds to our understanding of the biomechanical impact of cervical radiculopathy on chest pain, which has largely been overlooked during diagnostic workups. Once cervical radiculopathy has been identified, CA symptoms can be eased by alleviating the noxious input stemming from the pinched nerve roots.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
