M M Schneider, F Zimmermann, B Hollinger, A Zimmerer, K J Burkhart
{"title":"[自体髂骨骨移植经内侧入路治疗慢性肘关节不稳]。","authors":"M M Schneider, F Zimmermann, B Hollinger, A Zimmerer, K J Burkhart","doi":"10.1007/s00064-022-00783-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Neutralizing a posteromedial rotatory instability (PMRI) caused by coronoid deficiency by restoration of the humeroulnar joint surface with an autologous iliac crest bone graft.</p><p><strong>Indications: </strong>Surgery is indicated in patients with chronic deficiency of the anteromedial facet of the coronoid with subsequent PMRI.</p><p><strong>Contraindications: </strong>Coronoid reconstruction is not recommended in patients with advanced osteoarthritis of the elbow caused by subluxation of the humeroulnar joint. General contraindications like acute infection, pregnancy and lack of operability should also be taken into account.</p><p><strong>Surgical technique: </strong>First, a medial approach is established and the base of the coronoid is prepared. Afterwards an autologous iliac crest bone graft is placed onto the defect and secured by screws or a plate. In addition, a reconstruction of the anterior bundle of the medial collateral ligament with an autologous tendon graft is performed.</p><p><strong>Postoperative management: </strong>An elbow orthesis is worn for 6 weeks after surgery to avoid valgus or varus stress. There is no restriction in range of motion. A continuous passive motion elbow chair supports the patient in regaining elbow mobility.</p><p><strong>Results: </strong>Between 2015 and 2017, we treated 10 patients suffering from chronic coronoid defects with coronoid reconstruction. Eight of the patients were available for follow-up 86 weeks after surgery. The mean age was 41.4 years. In all patients, elbow range of motion and patient-related outcome measures were improved after surgery. Plain radiographs illustrated correct centering of the elbow joint. One patient had to undergo elbow arthroplasty and was excluded. Coronoid reconstruction with an autologous iliac crest bone graft restored humeroulnar joint congruency and improved satisfaction in patients suffering from chronic coronoid deficiency.</p>","PeriodicalId":54677,"journal":{"name":"Operative Orthopadie Und Traumatologie","volume":"34 6","pages":"419-430"},"PeriodicalIF":1.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9729130/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Coronoid reconstruction with autologous iliac crest bone graft in chronic elbow instability through a medial approach].\",\"authors\":\"M M Schneider, F Zimmermann, B Hollinger, A Zimmerer, K J Burkhart\",\"doi\":\"10.1007/s00064-022-00783-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Neutralizing a posteromedial rotatory instability (PMRI) caused by coronoid deficiency by restoration of the humeroulnar joint surface with an autologous iliac crest bone graft.</p><p><strong>Indications: </strong>Surgery is indicated in patients with chronic deficiency of the anteromedial facet of the coronoid with subsequent PMRI.</p><p><strong>Contraindications: </strong>Coronoid reconstruction is not recommended in patients with advanced osteoarthritis of the elbow caused by subluxation of the humeroulnar joint. General contraindications like acute infection, pregnancy and lack of operability should also be taken into account.</p><p><strong>Surgical technique: </strong>First, a medial approach is established and the base of the coronoid is prepared. Afterwards an autologous iliac crest bone graft is placed onto the defect and secured by screws or a plate. In addition, a reconstruction of the anterior bundle of the medial collateral ligament with an autologous tendon graft is performed.</p><p><strong>Postoperative management: </strong>An elbow orthesis is worn for 6 weeks after surgery to avoid valgus or varus stress. There is no restriction in range of motion. A continuous passive motion elbow chair supports the patient in regaining elbow mobility.</p><p><strong>Results: </strong>Between 2015 and 2017, we treated 10 patients suffering from chronic coronoid defects with coronoid reconstruction. Eight of the patients were available for follow-up 86 weeks after surgery. The mean age was 41.4 years. In all patients, elbow range of motion and patient-related outcome measures were improved after surgery. Plain radiographs illustrated correct centering of the elbow joint. One patient had to undergo elbow arthroplasty and was excluded. Coronoid reconstruction with an autologous iliac crest bone graft restored humeroulnar joint congruency and improved satisfaction in patients suffering from chronic coronoid deficiency.</p>\",\"PeriodicalId\":54677,\"journal\":{\"name\":\"Operative Orthopadie Und Traumatologie\",\"volume\":\"34 6\",\"pages\":\"419-430\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9729130/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Operative Orthopadie Und Traumatologie\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00064-022-00783-6\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Operative Orthopadie Und Traumatologie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00064-022-00783-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
[Coronoid reconstruction with autologous iliac crest bone graft in chronic elbow instability through a medial approach].
Objective: Neutralizing a posteromedial rotatory instability (PMRI) caused by coronoid deficiency by restoration of the humeroulnar joint surface with an autologous iliac crest bone graft.
Indications: Surgery is indicated in patients with chronic deficiency of the anteromedial facet of the coronoid with subsequent PMRI.
Contraindications: Coronoid reconstruction is not recommended in patients with advanced osteoarthritis of the elbow caused by subluxation of the humeroulnar joint. General contraindications like acute infection, pregnancy and lack of operability should also be taken into account.
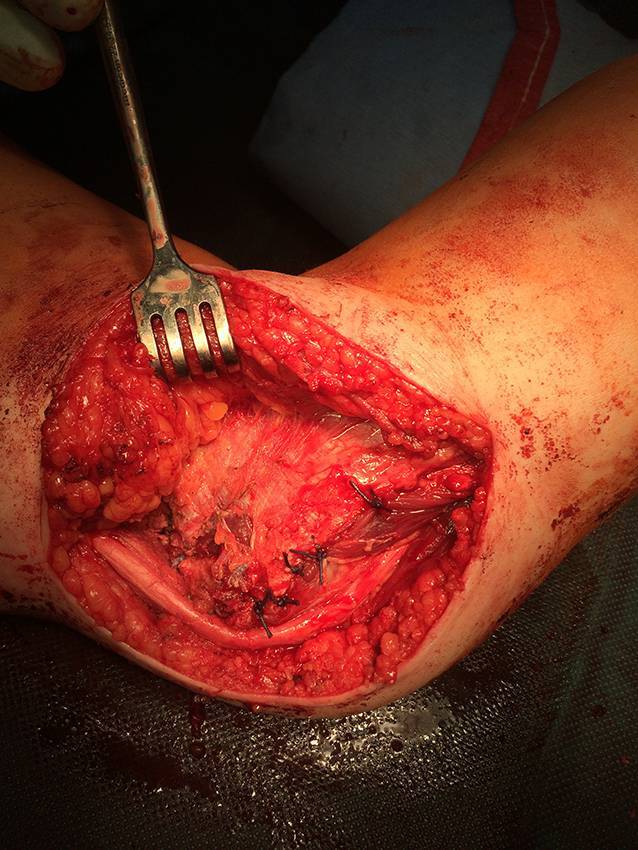
Surgical technique: First, a medial approach is established and the base of the coronoid is prepared. Afterwards an autologous iliac crest bone graft is placed onto the defect and secured by screws or a plate. In addition, a reconstruction of the anterior bundle of the medial collateral ligament with an autologous tendon graft is performed.
Postoperative management: An elbow orthesis is worn for 6 weeks after surgery to avoid valgus or varus stress. There is no restriction in range of motion. A continuous passive motion elbow chair supports the patient in regaining elbow mobility.
Results: Between 2015 and 2017, we treated 10 patients suffering from chronic coronoid defects with coronoid reconstruction. Eight of the patients were available for follow-up 86 weeks after surgery. The mean age was 41.4 years. In all patients, elbow range of motion and patient-related outcome measures were improved after surgery. Plain radiographs illustrated correct centering of the elbow joint. One patient had to undergo elbow arthroplasty and was excluded. Coronoid reconstruction with an autologous iliac crest bone graft restored humeroulnar joint congruency and improved satisfaction in patients suffering from chronic coronoid deficiency.
期刊介绍:
Orthopedics and Traumatology is directed toward all orthopedic surgeons, trauma-tologists, hand surgeons, specialists in sports injuries, orthopedics and rheumatology as well as gene-al surgeons who require access to reliable information on current operative methods to ensure the quality of patient advice, preoperative planning, and postoperative care.
The journal presents established and new operative procedures in uniformly structured and extensively illustrated contributions. All aspects are presented step-by-step from indications, contraindications, patient education, and preparation of the operation right through to postoperative care. The advantages and disadvantages, possible complications, deficiencies and risks of the methods as well as significant results with their evaluation criteria are discussed. To allow the reader to assess the outcome, results are detailed and based on internationally recognized scoring systems.
Orthopedics and Traumatology facilitates effective advancement and further education for all those active in both special and conservative fields of orthopedics, traumatology, and general surgery, offers sup-port for therapeutic decision-making, and provides – more than 30 years after its first publication – constantly expanding and up-to-date teaching on operative techniques.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
