Cairistin McDougall, Dana Wiens, Irene Smolik, Yvonne C Lee, Hani S El-Gabalawy, Liam J O'Neil
{"title":"超越视觉模拟量表:来自类风湿性关节炎患者一级亲属的多模态疼痛评估试点研究的结果。","authors":"Cairistin McDougall, Dana Wiens, Irene Smolik, Yvonne C Lee, Hani S El-Gabalawy, Liam J O'Neil","doi":"10.1002/acr2.11497","DOIUrl":null,"url":null,"abstract":"Pain is a universal phenomenon in individuals with rheumatoid arthritis (RA) occurring at all stages of the disease and remains a primary concern for most patients (1). In RA, painmay be due to inflammation, joint damage, peripheral sensitization, and central dysregulation of pain processing (2), but objectively measuring pain remains a challenge irrespective of the origin. The Visual Analog Scale (VAS) is the most commonly used tool to measure pain but provides no information on the neurobiological origin or intensity in varying locations. Quantitative sensory testing (QST) is a method to assess somatosensation using a variety of stimuli and collecting data based on the subjective experience of these stimuli. Reduced Pressure Pain Threshold (PPT) at joint sites is suggestive of peripheral sensitization, whereas widespread decreased PPT and increased mechanical Temporal Summation (TS) are suggestive of central sensitization (3). Despite a growing interest in the origins and assessment of pain, there is a paucity of data that aim to interrelate varying methodologies to measure pain. To better understand how to capture and quantify pain, we sought to undertake a multimodal pain assessment study using 1) a novel digital pain mapping tool, 2) QST, and 3) VAS pain score in patients with RA and their firstdegree relatives (FDRs). Both groups are known to experience higher levels of pain than the general population (4). In this pilot study, we enrolled 15 patients with RA and 14 FDRs of patients with RA who were part of a longitudinal cohort study of RA risk in First Nations people (n total = 29). We recorded baseline demographics including a 44 tender and swollen joint examination, pain VAS, and the modified health assessment questionnaire (mHAQ). QST, which included PPT and TS at multiple joint and nonjoint sites, was performed. PPT was assessed using a Wagner Force 10FDX Algometer at both joint sites (bilateral wrists and knees) and nonjoint sites (bilateral thumbs and trapezius muscles). TS was assessed at the left forearm using six calibrated, wire tipped probes of increasing weight (from 8 milliNewton [mN] to 256 mN). Participants completed a digital pain map using custom software on an Android Tablet to capture pain location and intensity on an electronic homunculus. Participants were able to choose a color hue on a scale of yellow to red to illustrate the intensity of their pain at each site, with yellow representing low intensity pain and red representing high intensity pain. Pain map scores were calculated using a weighted formula to account for intensity and area using ImageJ (range 1.2 to 144.8 AU). We analyzed the data using Wilcoxon signed rank test, χ, Spearman rank correlation, and linear regression where appropriate. This study was approved by the Research Ethics Board of the University of Manitoba (HS14453). The median age for FDRs and patients with RA were 43 and 44 years, respectively. Notably, seven of the patients with RA and five of the FDRs were using non-steroidal anti-inflammatory drugs (NSAIDs), whereas 11 patients with RA and six FDRs were using non-NSAID analgesics. The majority of the patients with RA were seropositive (13/15; 86.7%). There were no differences in trapezius PPT (4.62 IQR 2.96 to 5.75 kgf vs. 4.09 IQR 3.04 to 7.95; P = 0.631) (Figure 1A) or forearm TS (1.67 IQR 1.33 to 3.58 vs. 2.34 IQR 0.84 to 3.17; P = 0.497) (Figure 1B) between patients with RA and FDRs. Peripheral sensitization was also similar between patients with RA and FDRs with no apparent differences in joint and nonjoint PPT (all P values > 0.05). VAS pain was higher in patients with RA (64 IQR 34.5 to 79.0) compared with FDRs (29 IQR 20.8 to 77.8; P = 0.335) (Figure 1C). Despite the small scale of this feasibility study, digital pain map scores were significantly higher in patients with RA (29.7 IQR 21.2 to 45.3) compared with FDRs (8.7 IQR 4.6 to 20.9; P = 0.009) (Figure 1D). Interestingly, pain map score was only weakly associated with pain VAS (R = 0.23; P = 0.24) and not associated with forearm TS (R = −0.09; P = 0.635) or trapezius PPT (R = 0.07; P = 0.725). However, pain map score correlated strongly with mHAQ score, a standardized measure of functional disability (R = 0.78; P < 0.001) (Figure 1E). No association between PPT or TS and mHAQ was observed (R = −0.16; R = 0.28, respectively). Pain VAS correlated modestly with mHAQ (R = 0.38; P = 0.05). Using linear regression, we found that only pain map score was independently associated with mHAQ after controlling for analgesia use (NSAID/non-NSAID) and RA diagnosis (ß = 1.26; 0.58 to 1.95; P = 0.0008). We conclude that a multimodal pain assessment protocol is feasible, and that of all the modalities tested, pain map score was most valuable for identifying RA-specific pain, which was also closely associated with functional disability, a key outcome measure for patients with RA. It is important to note limitations of this study. The protocol was designed as a pilot study to attempt to understand the feasibility of performing a broad, multimodal pain assessment in a clinically","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"4 12","pages":"1027-1029"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/38/41/ACR2-4-1027.PMC9746659.pdf","citationCount":"0","resultStr":"{\"title\":\"Beyond the visual analog scale: results from a multimodal pain assessment pilot study in first-degree relatives of patients with rheumatoid arthritis.\",\"authors\":\"Cairistin McDougall, Dana Wiens, Irene Smolik, Yvonne C Lee, Hani S El-Gabalawy, Liam J O'Neil\",\"doi\":\"10.1002/acr2.11497\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Pain is a universal phenomenon in individuals with rheumatoid arthritis (RA) occurring at all stages of the disease and remains a primary concern for most patients (1). In RA, painmay be due to inflammation, joint damage, peripheral sensitization, and central dysregulation of pain processing (2), but objectively measuring pain remains a challenge irrespective of the origin. The Visual Analog Scale (VAS) is the most commonly used tool to measure pain but provides no information on the neurobiological origin or intensity in varying locations. Quantitative sensory testing (QST) is a method to assess somatosensation using a variety of stimuli and collecting data based on the subjective experience of these stimuli. Reduced Pressure Pain Threshold (PPT) at joint sites is suggestive of peripheral sensitization, whereas widespread decreased PPT and increased mechanical Temporal Summation (TS) are suggestive of central sensitization (3). Despite a growing interest in the origins and assessment of pain, there is a paucity of data that aim to interrelate varying methodologies to measure pain. To better understand how to capture and quantify pain, we sought to undertake a multimodal pain assessment study using 1) a novel digital pain mapping tool, 2) QST, and 3) VAS pain score in patients with RA and their firstdegree relatives (FDRs). Both groups are known to experience higher levels of pain than the general population (4). In this pilot study, we enrolled 15 patients with RA and 14 FDRs of patients with RA who were part of a longitudinal cohort study of RA risk in First Nations people (n total = 29). We recorded baseline demographics including a 44 tender and swollen joint examination, pain VAS, and the modified health assessment questionnaire (mHAQ). QST, which included PPT and TS at multiple joint and nonjoint sites, was performed. PPT was assessed using a Wagner Force 10FDX Algometer at both joint sites (bilateral wrists and knees) and nonjoint sites (bilateral thumbs and trapezius muscles). TS was assessed at the left forearm using six calibrated, wire tipped probes of increasing weight (from 8 milliNewton [mN] to 256 mN). Participants completed a digital pain map using custom software on an Android Tablet to capture pain location and intensity on an electronic homunculus. Participants were able to choose a color hue on a scale of yellow to red to illustrate the intensity of their pain at each site, with yellow representing low intensity pain and red representing high intensity pain. Pain map scores were calculated using a weighted formula to account for intensity and area using ImageJ (range 1.2 to 144.8 AU). We analyzed the data using Wilcoxon signed rank test, χ, Spearman rank correlation, and linear regression where appropriate. This study was approved by the Research Ethics Board of the University of Manitoba (HS14453). The median age for FDRs and patients with RA were 43 and 44 years, respectively. Notably, seven of the patients with RA and five of the FDRs were using non-steroidal anti-inflammatory drugs (NSAIDs), whereas 11 patients with RA and six FDRs were using non-NSAID analgesics. The majority of the patients with RA were seropositive (13/15; 86.7%). There were no differences in trapezius PPT (4.62 IQR 2.96 to 5.75 kgf vs. 4.09 IQR 3.04 to 7.95; P = 0.631) (Figure 1A) or forearm TS (1.67 IQR 1.33 to 3.58 vs. 2.34 IQR 0.84 to 3.17; P = 0.497) (Figure 1B) between patients with RA and FDRs. Peripheral sensitization was also similar between patients with RA and FDRs with no apparent differences in joint and nonjoint PPT (all P values > 0.05). VAS pain was higher in patients with RA (64 IQR 34.5 to 79.0) compared with FDRs (29 IQR 20.8 to 77.8; P = 0.335) (Figure 1C). Despite the small scale of this feasibility study, digital pain map scores were significantly higher in patients with RA (29.7 IQR 21.2 to 45.3) compared with FDRs (8.7 IQR 4.6 to 20.9; P = 0.009) (Figure 1D). Interestingly, pain map score was only weakly associated with pain VAS (R = 0.23; P = 0.24) and not associated with forearm TS (R = −0.09; P = 0.635) or trapezius PPT (R = 0.07; P = 0.725). However, pain map score correlated strongly with mHAQ score, a standardized measure of functional disability (R = 0.78; P < 0.001) (Figure 1E). No association between PPT or TS and mHAQ was observed (R = −0.16; R = 0.28, respectively). Pain VAS correlated modestly with mHAQ (R = 0.38; P = 0.05). Using linear regression, we found that only pain map score was independently associated with mHAQ after controlling for analgesia use (NSAID/non-NSAID) and RA diagnosis (ß = 1.26; 0.58 to 1.95; P = 0.0008). We conclude that a multimodal pain assessment protocol is feasible, and that of all the modalities tested, pain map score was most valuable for identifying RA-specific pain, which was also closely associated with functional disability, a key outcome measure for patients with RA. It is important to note limitations of this study. The protocol was designed as a pilot study to attempt to understand the feasibility of performing a broad, multimodal pain assessment in a clinically\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\"4 12\",\"pages\":\"1027-1029\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/38/41/ACR2-4-1027.PMC9746659.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11497\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11497","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Beyond the visual analog scale: results from a multimodal pain assessment pilot study in first-degree relatives of patients with rheumatoid arthritis.
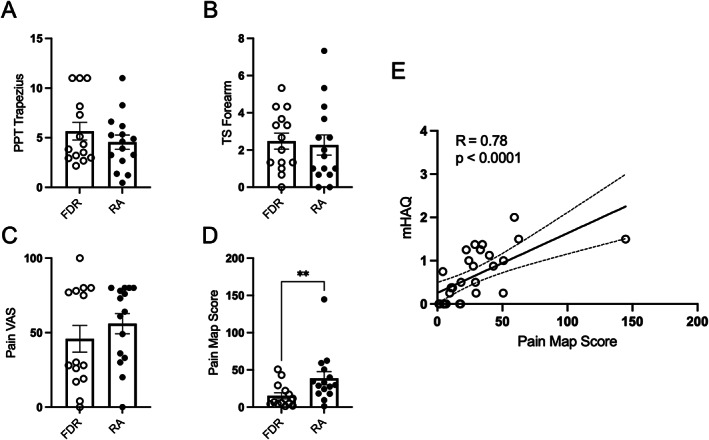
Pain is a universal phenomenon in individuals with rheumatoid arthritis (RA) occurring at all stages of the disease and remains a primary concern for most patients (1). In RA, painmay be due to inflammation, joint damage, peripheral sensitization, and central dysregulation of pain processing (2), but objectively measuring pain remains a challenge irrespective of the origin. The Visual Analog Scale (VAS) is the most commonly used tool to measure pain but provides no information on the neurobiological origin or intensity in varying locations. Quantitative sensory testing (QST) is a method to assess somatosensation using a variety of stimuli and collecting data based on the subjective experience of these stimuli. Reduced Pressure Pain Threshold (PPT) at joint sites is suggestive of peripheral sensitization, whereas widespread decreased PPT and increased mechanical Temporal Summation (TS) are suggestive of central sensitization (3). Despite a growing interest in the origins and assessment of pain, there is a paucity of data that aim to interrelate varying methodologies to measure pain. To better understand how to capture and quantify pain, we sought to undertake a multimodal pain assessment study using 1) a novel digital pain mapping tool, 2) QST, and 3) VAS pain score in patients with RA and their firstdegree relatives (FDRs). Both groups are known to experience higher levels of pain than the general population (4). In this pilot study, we enrolled 15 patients with RA and 14 FDRs of patients with RA who were part of a longitudinal cohort study of RA risk in First Nations people (n total = 29). We recorded baseline demographics including a 44 tender and swollen joint examination, pain VAS, and the modified health assessment questionnaire (mHAQ). QST, which included PPT and TS at multiple joint and nonjoint sites, was performed. PPT was assessed using a Wagner Force 10FDX Algometer at both joint sites (bilateral wrists and knees) and nonjoint sites (bilateral thumbs and trapezius muscles). TS was assessed at the left forearm using six calibrated, wire tipped probes of increasing weight (from 8 milliNewton [mN] to 256 mN). Participants completed a digital pain map using custom software on an Android Tablet to capture pain location and intensity on an electronic homunculus. Participants were able to choose a color hue on a scale of yellow to red to illustrate the intensity of their pain at each site, with yellow representing low intensity pain and red representing high intensity pain. Pain map scores were calculated using a weighted formula to account for intensity and area using ImageJ (range 1.2 to 144.8 AU). We analyzed the data using Wilcoxon signed rank test, χ, Spearman rank correlation, and linear regression where appropriate. This study was approved by the Research Ethics Board of the University of Manitoba (HS14453). The median age for FDRs and patients with RA were 43 and 44 years, respectively. Notably, seven of the patients with RA and five of the FDRs were using non-steroidal anti-inflammatory drugs (NSAIDs), whereas 11 patients with RA and six FDRs were using non-NSAID analgesics. The majority of the patients with RA were seropositive (13/15; 86.7%). There were no differences in trapezius PPT (4.62 IQR 2.96 to 5.75 kgf vs. 4.09 IQR 3.04 to 7.95; P = 0.631) (Figure 1A) or forearm TS (1.67 IQR 1.33 to 3.58 vs. 2.34 IQR 0.84 to 3.17; P = 0.497) (Figure 1B) between patients with RA and FDRs. Peripheral sensitization was also similar between patients with RA and FDRs with no apparent differences in joint and nonjoint PPT (all P values > 0.05). VAS pain was higher in patients with RA (64 IQR 34.5 to 79.0) compared with FDRs (29 IQR 20.8 to 77.8; P = 0.335) (Figure 1C). Despite the small scale of this feasibility study, digital pain map scores were significantly higher in patients with RA (29.7 IQR 21.2 to 45.3) compared with FDRs (8.7 IQR 4.6 to 20.9; P = 0.009) (Figure 1D). Interestingly, pain map score was only weakly associated with pain VAS (R = 0.23; P = 0.24) and not associated with forearm TS (R = −0.09; P = 0.635) or trapezius PPT (R = 0.07; P = 0.725). However, pain map score correlated strongly with mHAQ score, a standardized measure of functional disability (R = 0.78; P < 0.001) (Figure 1E). No association between PPT or TS and mHAQ was observed (R = −0.16; R = 0.28, respectively). Pain VAS correlated modestly with mHAQ (R = 0.38; P = 0.05). Using linear regression, we found that only pain map score was independently associated with mHAQ after controlling for analgesia use (NSAID/non-NSAID) and RA diagnosis (ß = 1.26; 0.58 to 1.95; P = 0.0008). We conclude that a multimodal pain assessment protocol is feasible, and that of all the modalities tested, pain map score was most valuable for identifying RA-specific pain, which was also closely associated with functional disability, a key outcome measure for patients with RA. It is important to note limitations of this study. The protocol was designed as a pilot study to attempt to understand the feasibility of performing a broad, multimodal pain assessment in a clinically


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
