{"title":"临床表现:泪腺炎伴免疫球蛋白g4相关疾病的嗜酸性肉芽肿病伴多血管炎。","authors":"Sho Ishigaki, Mitsuhiro Akiyama","doi":"10.1002/acr2.11508","DOIUrl":null,"url":null,"abstract":"The patient, a 26-year-old woman, presented with a 2-week history of acute swelling in both lacrimal glands ( A ). She had recently developed uncontrolled asthma and nasal polyps. The laboratory test results were notable for an absolute eosinophil count of 5300 cells per μ l (reference range 100-400 μ l), exceeding 50% of circulating leukocytes. The antineutrophil cytoplasmic antibody test result was negative. Magnetic resonance imaging of the head con fi rmed swelling of the bilateral lacrimal glands ( B , yellow arrowheads) and rhinosi-nusitis. A biopsy of her lacrimal gland revealed eosinophil-rich necrotizing granulomatous in fl ammation with vasculitis ( C ). Her serum immunoglobulin G4 (IgG4) level was slightly elevated (265 mg/dl, normal upper limit is 121 mg/dl), but IgG4 immunostaining of the biopsy specimen did not show a signi fi cant fi nding. A diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) was made. Treatment with 30 mg of prednisone was initiated, which was gradually tapered without glucocorticoid-sparing agents over 12 months. The swelling of her lacrimal glands resolved, and she was free of symptoms, including asthma and lacrimal gland swelling, at the 12-month follow-up. In summary, EGPA can present with lacrimal gland swelling and mimic IgG4-related Mikulicz disease (1,2). A histopathological examination of the swollen lacrimal gland is the key to differentiating EGPA from IgG4-related Mikulicz disease in such cases. Author disclosures","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"4 12","pages":"1030"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/3a/ACR2-4-1030.PMC9746660.pdf","citationCount":"1","resultStr":"{\"title\":\"Clinical Images: Dacryoadenitis in eosinophilic granulomatosis with polyangiitis mimicking immunoglobulin G4-related disease.\",\"authors\":\"Sho Ishigaki, Mitsuhiro Akiyama\",\"doi\":\"10.1002/acr2.11508\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"The patient, a 26-year-old woman, presented with a 2-week history of acute swelling in both lacrimal glands ( A ). She had recently developed uncontrolled asthma and nasal polyps. The laboratory test results were notable for an absolute eosinophil count of 5300 cells per μ l (reference range 100-400 μ l), exceeding 50% of circulating leukocytes. The antineutrophil cytoplasmic antibody test result was negative. Magnetic resonance imaging of the head con fi rmed swelling of the bilateral lacrimal glands ( B , yellow arrowheads) and rhinosi-nusitis. A biopsy of her lacrimal gland revealed eosinophil-rich necrotizing granulomatous in fl ammation with vasculitis ( C ). Her serum immunoglobulin G4 (IgG4) level was slightly elevated (265 mg/dl, normal upper limit is 121 mg/dl), but IgG4 immunostaining of the biopsy specimen did not show a signi fi cant fi nding. A diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) was made. Treatment with 30 mg of prednisone was initiated, which was gradually tapered without glucocorticoid-sparing agents over 12 months. The swelling of her lacrimal glands resolved, and she was free of symptoms, including asthma and lacrimal gland swelling, at the 12-month follow-up. In summary, EGPA can present with lacrimal gland swelling and mimic IgG4-related Mikulicz disease (1,2). A histopathological examination of the swollen lacrimal gland is the key to differentiating EGPA from IgG4-related Mikulicz disease in such cases. Author disclosures\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\"4 12\",\"pages\":\"1030\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/3a/ACR2-4-1030.PMC9746660.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11508\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11508","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical Images: Dacryoadenitis in eosinophilic granulomatosis with polyangiitis mimicking immunoglobulin G4-related disease.
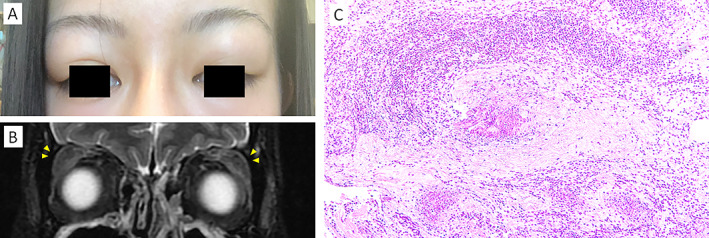
The patient, a 26-year-old woman, presented with a 2-week history of acute swelling in both lacrimal glands ( A ). She had recently developed uncontrolled asthma and nasal polyps. The laboratory test results were notable for an absolute eosinophil count of 5300 cells per μ l (reference range 100-400 μ l), exceeding 50% of circulating leukocytes. The antineutrophil cytoplasmic antibody test result was negative. Magnetic resonance imaging of the head con fi rmed swelling of the bilateral lacrimal glands ( B , yellow arrowheads) and rhinosi-nusitis. A biopsy of her lacrimal gland revealed eosinophil-rich necrotizing granulomatous in fl ammation with vasculitis ( C ). Her serum immunoglobulin G4 (IgG4) level was slightly elevated (265 mg/dl, normal upper limit is 121 mg/dl), but IgG4 immunostaining of the biopsy specimen did not show a signi fi cant fi nding. A diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) was made. Treatment with 30 mg of prednisone was initiated, which was gradually tapered without glucocorticoid-sparing agents over 12 months. The swelling of her lacrimal glands resolved, and she was free of symptoms, including asthma and lacrimal gland swelling, at the 12-month follow-up. In summary, EGPA can present with lacrimal gland swelling and mimic IgG4-related Mikulicz disease (1,2). A histopathological examination of the swollen lacrimal gland is the key to differentiating EGPA from IgG4-related Mikulicz disease in such cases. Author disclosures



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
