Jessica Atwell, Martha Chico, Maritza Vaca, Andrea Arévalo-Cortes, Ruth Karron, Philip J. Cooper
{"title":"非工业化环境下婴儿病毒性呼吸道疾病对儿童哮喘的影响","authors":"Jessica Atwell, Martha Chico, Maritza Vaca, Andrea Arévalo-Cortes, Ruth Karron, Philip J. Cooper","doi":"10.1002/clt2.12291","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>There are limited data from non-industrialized settings on the effects of early life viral respiratory disease on childhood respiratory illness. We followed a birth cohort in tropical Ecuador to understand how early viral respiratory disease, in the context of exposures affecting airway inflammation including ascariasis, affect wheezing illness, asthma, and rhinoconjunctivitis in later childhood.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A surveillance cohort nested within a birth cohort was monitored for respiratory infections during the first 2 years in rural Ecuador and followed for 8 years for the development of wheeze and rhinoconjunctivitis. Nasal swabs were examined for viruses by polymerase chain reaction and respiratory symptom data on recent wheeze and rhinoconjunctivitis were collected by periodic questionnaires at 3, 5, and 8 years. Stools from pregnant mothers and periodically from children aged 2 years were examined microscopically for soil-transmitted helminths. Atopy was measured by allergen skin prick testing at 2 years. Spirometry, fractional exhaled nitric oxide measurement, and nasal washes were performed at 8 years. Associations between clinically significant respiratory disease (CSRD) and wheezing or rhinoconjunctivitis at 3, 5, and 8 years were estimated using multivariable logistic regression.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Four hundred and twenty six children were followed of which 67.7% had at least one CSRD episode; 12% had respiratory syncytial virus (RSV)+CSRD and 36% had rhinovirus (RHV)+CSRD. All-cause CSRD was associated with increased wheeze at 3 (OR 2.33 [95% confidence intervals (CI) 1.23–4.40]) and 5 (OR: 2.12 [95% CI 1.12–4.01]) years. RHV+CSRD was more strongly associated with wheeze at 3 years in STH-infected (STH-infected [OR 13.41, 95% CI 1.56–115.64] vs. uninfected [OR 1.68, 95% CI 0.73–3.84]) and SPT+ (SPT+ [OR 9.42, 95% CI 1.88–47.15] versus SPT- [OR 1.92, 95% CI 0.84–4.38]) children. No associations were observed between CSRD and rhinoconjunctivitis.</p>\n </section>\n \n <section>\n \n <h3> Discussion</h3>\n \n <p>CSRD was significantly associated with childhood wheeze with stronger associations observed for RHV+CSRD in SPT+ and STH-infected children.</p>\n </section>\n </div>","PeriodicalId":10334,"journal":{"name":"Clinical and Translational Allergy","volume":"13 8","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2023-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.12291","citationCount":"0","resultStr":"{\"title\":\"Effect of infant viral respiratory disease on childhood asthma in a non-industrialized setting\",\"authors\":\"Jessica Atwell, Martha Chico, Maritza Vaca, Andrea Arévalo-Cortes, Ruth Karron, Philip J. Cooper\",\"doi\":\"10.1002/clt2.12291\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>There are limited data from non-industrialized settings on the effects of early life viral respiratory disease on childhood respiratory illness. We followed a birth cohort in tropical Ecuador to understand how early viral respiratory disease, in the context of exposures affecting airway inflammation including ascariasis, affect wheezing illness, asthma, and rhinoconjunctivitis in later childhood.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A surveillance cohort nested within a birth cohort was monitored for respiratory infections during the first 2 years in rural Ecuador and followed for 8 years for the development of wheeze and rhinoconjunctivitis. Nasal swabs were examined for viruses by polymerase chain reaction and respiratory symptom data on recent wheeze and rhinoconjunctivitis were collected by periodic questionnaires at 3, 5, and 8 years. Stools from pregnant mothers and periodically from children aged 2 years were examined microscopically for soil-transmitted helminths. Atopy was measured by allergen skin prick testing at 2 years. Spirometry, fractional exhaled nitric oxide measurement, and nasal washes were performed at 8 years. Associations between clinically significant respiratory disease (CSRD) and wheezing or rhinoconjunctivitis at 3, 5, and 8 years were estimated using multivariable logistic regression.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Four hundred and twenty six children were followed of which 67.7% had at least one CSRD episode; 12% had respiratory syncytial virus (RSV)+CSRD and 36% had rhinovirus (RHV)+CSRD. All-cause CSRD was associated with increased wheeze at 3 (OR 2.33 [95% confidence intervals (CI) 1.23–4.40]) and 5 (OR: 2.12 [95% CI 1.12–4.01]) years. RHV+CSRD was more strongly associated with wheeze at 3 years in STH-infected (STH-infected [OR 13.41, 95% CI 1.56–115.64] vs. uninfected [OR 1.68, 95% CI 0.73–3.84]) and SPT+ (SPT+ [OR 9.42, 95% CI 1.88–47.15] versus SPT- [OR 1.92, 95% CI 0.84–4.38]) children. No associations were observed between CSRD and rhinoconjunctivitis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Discussion</h3>\\n \\n <p>CSRD was significantly associated with childhood wheeze with stronger associations observed for RHV+CSRD in SPT+ and STH-infected children.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10334,\"journal\":{\"name\":\"Clinical and Translational Allergy\",\"volume\":\"13 8\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.12291\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12291\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12291","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
摘要
关于早期病毒性呼吸道疾病对儿童呼吸道疾病的影响,来自非工业化环境的数据有限。我们跟踪了厄瓜多尔热带地区的一个出生队列,以了解早期病毒性呼吸道疾病是如何影响包括蛔虫病在内的气道炎症,影响儿童后期的喘息性疾病、哮喘和鼻结膜炎。方法对厄瓜多尔农村出生队列中嵌套的监测队列进行前2年的呼吸道感染监测,并对其进行8年的喘息和鼻结膜炎的随访。采用聚合酶链反应法检测鼻拭子病毒,并在3、5和8岁时通过定期问卷收集最近喘息和鼻结膜炎的呼吸道症状数据。在显微镜下检查孕妇和2岁儿童的粪便中是否有土壤传播的蠕虫。2岁时,通过过敏原皮肤点刺试验测量变态反应性。8岁时进行肺活量测定、呼气一氧化氮分数测定和鼻洗。使用多变量logistic回归估计临床显著呼吸系统疾病(CSRD)与喘息或鼻结膜炎在3、5和8年时的相关性。结果随访426例患儿,其中67.7%至少有一次CSRD发作;呼吸道合胞病毒(RSV)+CSRD占12%,鼻病毒(RHV)+CSRD占36%。全因CSRD在3年(OR 2.33[95%可信区间(CI) 1.23-4.40])和5年(OR: 2.12 [95% CI 1.12-4.01])时与喘息增加相关。在sth感染(sth感染[OR 13.41, 95% CI 1.56-115.64] vs.未感染[OR 1.68, 95% CI 0.73-3.84])和SPT+ (SPT+ [OR 9.42, 95% CI 1.88-47.15] vs. SPT- [OR 1.92, 95% CI 0.84-4.38])儿童中,RHV+CSRD与3岁时喘息的相关性更强。未观察到CSRD与鼻结膜炎之间的关联。CSRD与儿童喘息显著相关,在SPT+和sth感染的儿童中观察到RHV+CSRD的相关性更强。
Effect of infant viral respiratory disease on childhood asthma in a non-industrialized setting
Background
There are limited data from non-industrialized settings on the effects of early life viral respiratory disease on childhood respiratory illness. We followed a birth cohort in tropical Ecuador to understand how early viral respiratory disease, in the context of exposures affecting airway inflammation including ascariasis, affect wheezing illness, asthma, and rhinoconjunctivitis in later childhood.
Methods
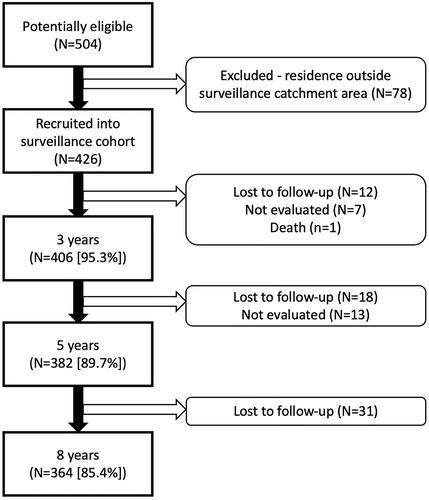
A surveillance cohort nested within a birth cohort was monitored for respiratory infections during the first 2 years in rural Ecuador and followed for 8 years for the development of wheeze and rhinoconjunctivitis. Nasal swabs were examined for viruses by polymerase chain reaction and respiratory symptom data on recent wheeze and rhinoconjunctivitis were collected by periodic questionnaires at 3, 5, and 8 years. Stools from pregnant mothers and periodically from children aged 2 years were examined microscopically for soil-transmitted helminths. Atopy was measured by allergen skin prick testing at 2 years. Spirometry, fractional exhaled nitric oxide measurement, and nasal washes were performed at 8 years. Associations between clinically significant respiratory disease (CSRD) and wheezing or rhinoconjunctivitis at 3, 5, and 8 years were estimated using multivariable logistic regression.
Results
Four hundred and twenty six children were followed of which 67.7% had at least one CSRD episode; 12% had respiratory syncytial virus (RSV)+CSRD and 36% had rhinovirus (RHV)+CSRD. All-cause CSRD was associated with increased wheeze at 3 (OR 2.33 [95% confidence intervals (CI) 1.23–4.40]) and 5 (OR: 2.12 [95% CI 1.12–4.01]) years. RHV+CSRD was more strongly associated with wheeze at 3 years in STH-infected (STH-infected [OR 13.41, 95% CI 1.56–115.64] vs. uninfected [OR 1.68, 95% CI 0.73–3.84]) and SPT+ (SPT+ [OR 9.42, 95% CI 1.88–47.15] versus SPT- [OR 1.92, 95% CI 0.84–4.38]) children. No associations were observed between CSRD and rhinoconjunctivitis.
Discussion
CSRD was significantly associated with childhood wheeze with stronger associations observed for RHV+CSRD in SPT+ and STH-infected children.
期刊介绍:
Clinical and Translational Allergy, one of several journals in the portfolio of the European Academy of Allergy and Clinical Immunology, provides a platform for the dissemination of allergy research and reviews, as well as EAACI position papers, task force reports and guidelines, amongst an international scientific audience.
Clinical and Translational Allergy accepts clinical and translational research in the following areas and other related topics: asthma, rhinitis, rhinosinusitis, drug hypersensitivity, allergic conjunctivitis, allergic skin diseases, atopic eczema, urticaria, angioedema, venom hypersensitivity, anaphylaxis, food allergy, immunotherapy, immune modulators and biologics, animal models of allergic disease, immune mechanisms, or any other topic related to allergic disease.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
