Gift Mulima, Stein Atle Lie, Anthony Charles, Asma Bilal Hanif, Carlos G Varela, Leonard N Banza, Sven Young
{"title":"马拉维三级转诊医院创伤性脑损伤患者气管切开术无机械通气:一项横断面研究","authors":"Gift Mulima, Stein Atle Lie, Anthony Charles, Asma Bilal Hanif, Carlos G Varela, Leonard N Banza, Sven Young","doi":"10.4314/mmj.v34i3.2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tracheostomy alone, without mechanical ventilation, has been advocated to maintain a free airway in patients with traumatic brain injury in low-income settings with minimal critical care capacity. However, no reports exist on the outcomes of this strategy. We examine the results of this practice at a central hospital in Malawi.</p><p><strong>Methods: </strong>This is a retrospective review of medical records and prospectively gathered trauma surveillance data of patients admitted to Kamuzu Central Hospital, with traumatic brain injury from January 2010 to December 2015. In-hospital mortality rates were examined according to registered traumatic brain injury severity and airway management.</p><p><strong>Results: </strong>In our analysis, 1875 of 2051 registered traumatic brain injury patients were included; 83.3% were male, mean age 32.6 (SD 12.9) years. 14.2% (n=267) of the patients had invasive airway management (endotracheal tube or tracheostomy) with or without mechanical ventilation. Mortality in severe traumatic brain injury treated with tracheostomy without mechanical ventilation was 42% (10/24) compared to 21% (14/68) in patients treated without intubation or tracheostomy (p= 0.043). Tracheostomies had an overall complication rate of 11%.</p><p><strong>Conclusion: </strong>Tracheostomy without mechanical ventilation in severe traumatic brain injury did not improve survival outcomes in our setting. Tracheostomy for severe traumatic brain injury cannot be recommended when mechanical ventilation is not available unless there are sufficient specialized human resources for follow up in the ward. Efforts to improve critical care facilities and human resource capacity to allow proper use of mechanical ventilation in severe traumatic brain injury should be a high priority in low-income countries where the burden of trauma is high.</p>","PeriodicalId":18185,"journal":{"name":"Malawi Medical Journal","volume":"34 3","pages":"152-156"},"PeriodicalIF":0.8000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/93/53/MMJ3403-0152.PMC9641605.pdf","citationCount":"0","resultStr":"{\"title\":\"Tracheostomy without mechanical ventilation in patients with traumatic brain injury at a tertiary referral hospital in Malawi: a cross sectional study.\",\"authors\":\"Gift Mulima, Stein Atle Lie, Anthony Charles, Asma Bilal Hanif, Carlos G Varela, Leonard N Banza, Sven Young\",\"doi\":\"10.4314/mmj.v34i3.2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Tracheostomy alone, without mechanical ventilation, has been advocated to maintain a free airway in patients with traumatic brain injury in low-income settings with minimal critical care capacity. However, no reports exist on the outcomes of this strategy. We examine the results of this practice at a central hospital in Malawi.</p><p><strong>Methods: </strong>This is a retrospective review of medical records and prospectively gathered trauma surveillance data of patients admitted to Kamuzu Central Hospital, with traumatic brain injury from January 2010 to December 2015. In-hospital mortality rates were examined according to registered traumatic brain injury severity and airway management.</p><p><strong>Results: </strong>In our analysis, 1875 of 2051 registered traumatic brain injury patients were included; 83.3% were male, mean age 32.6 (SD 12.9) years. 14.2% (n=267) of the patients had invasive airway management (endotracheal tube or tracheostomy) with or without mechanical ventilation. Mortality in severe traumatic brain injury treated with tracheostomy without mechanical ventilation was 42% (10/24) compared to 21% (14/68) in patients treated without intubation or tracheostomy (p= 0.043). Tracheostomies had an overall complication rate of 11%.</p><p><strong>Conclusion: </strong>Tracheostomy without mechanical ventilation in severe traumatic brain injury did not improve survival outcomes in our setting. Tracheostomy for severe traumatic brain injury cannot be recommended when mechanical ventilation is not available unless there are sufficient specialized human resources for follow up in the ward. Efforts to improve critical care facilities and human resource capacity to allow proper use of mechanical ventilation in severe traumatic brain injury should be a high priority in low-income countries where the burden of trauma is high.</p>\",\"PeriodicalId\":18185,\"journal\":{\"name\":\"Malawi Medical Journal\",\"volume\":\"34 3\",\"pages\":\"152-156\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/93/53/MMJ3403-0152.PMC9641605.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Malawi Medical Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4314/mmj.v34i3.2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Malawi Medical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4314/mmj.v34i3.2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Tracheostomy without mechanical ventilation in patients with traumatic brain injury at a tertiary referral hospital in Malawi: a cross sectional study.
Background: Tracheostomy alone, without mechanical ventilation, has been advocated to maintain a free airway in patients with traumatic brain injury in low-income settings with minimal critical care capacity. However, no reports exist on the outcomes of this strategy. We examine the results of this practice at a central hospital in Malawi.
Methods: This is a retrospective review of medical records and prospectively gathered trauma surveillance data of patients admitted to Kamuzu Central Hospital, with traumatic brain injury from January 2010 to December 2015. In-hospital mortality rates were examined according to registered traumatic brain injury severity and airway management.
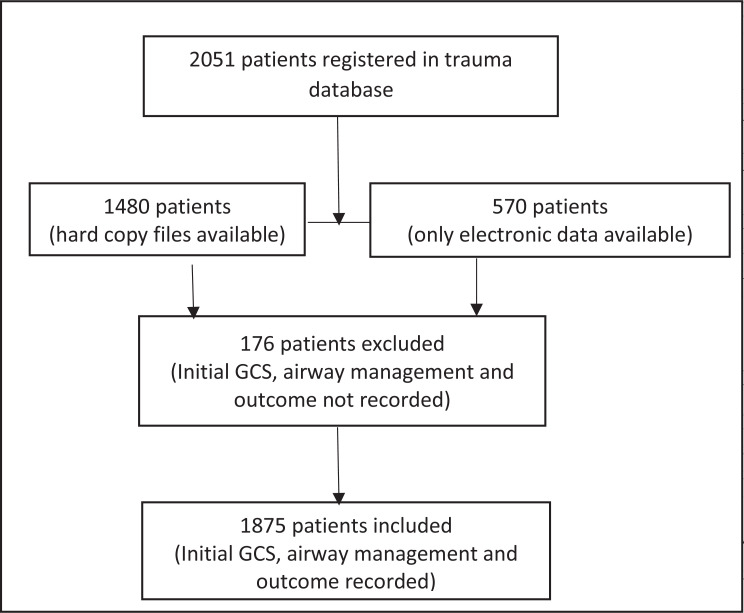
Results: In our analysis, 1875 of 2051 registered traumatic brain injury patients were included; 83.3% were male, mean age 32.6 (SD 12.9) years. 14.2% (n=267) of the patients had invasive airway management (endotracheal tube or tracheostomy) with or without mechanical ventilation. Mortality in severe traumatic brain injury treated with tracheostomy without mechanical ventilation was 42% (10/24) compared to 21% (14/68) in patients treated without intubation or tracheostomy (p= 0.043). Tracheostomies had an overall complication rate of 11%.
Conclusion: Tracheostomy without mechanical ventilation in severe traumatic brain injury did not improve survival outcomes in our setting. Tracheostomy for severe traumatic brain injury cannot be recommended when mechanical ventilation is not available unless there are sufficient specialized human resources for follow up in the ward. Efforts to improve critical care facilities and human resource capacity to allow proper use of mechanical ventilation in severe traumatic brain injury should be a high priority in low-income countries where the burden of trauma is high.
期刊介绍:
Driven and guided by the priorities articulated in the Malawi National Health Research Agenda, the Malawi Medical Journal publishes original research, short reports, case reports, viewpoints, insightful editorials and commentaries that are of high quality, informative and applicable to the Malawian and sub-Saharan Africa regions. Our particular interest is to publish evidence-based research that impacts and informs national health policies and medical practice in Malawi and the broader region.
Topics covered in the journal include, but are not limited to:
- Communicable diseases (HIV and AIDS, Malaria, TB, etc.)
- Non-communicable diseases (Cardiovascular diseases, cancer, diabetes, etc.)
- Sexual and Reproductive Health (Adolescent health, education, pregnancy and abortion, STDs and HIV and AIDS, etc.)
- Mental health
- Environmental health
- Nutrition
- Health systems and health policy (Leadership, ethics, and governance)
- Community systems strengthening research
- Injury, trauma, and surgical disorders



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
