Haoxun Tang, Xin Guo, Xiaolu Nie, Lin Zheng, Gang Liu, Wilfred Hing-Sang Wong, Yiu-Fai Cheung
{"title":"解释发热儿童冠状动脉尺寸的表象图法。","authors":"Haoxun Tang, Xin Guo, Xiaolu Nie, Lin Zheng, Gang Liu, Wilfred Hing-Sang Wong, Yiu-Fai Cheung","doi":"10.1002/ped4.12361","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Coronary artery dilation may occur in febrile children with and without Kawasaki disease (KD).</p><p><strong>Objective: </strong>We explored the application of unsupervised learning algorithms in the detection of novel patterns of coronary artery phenotypes in febrile children with and without KD.</p><p><strong>Methods: </strong>A total of 239 febrile children (59 non-KD and 180 KD patients), were recruited. Unsupervised hierarchical clustering analysis of phenotypic data including age, hemoglobin, white cell count, platelet count, C-reactive protein, erythrocyte sedimentation rate, albumin, alanine aminotransferase, aspartate aminotransferase, and coronary artery <i>z</i> scores were performed.</p><p><strong>Results: </strong>Using a cutoff <i>z</i> score of 2.5, the specificity was 98.3% and the sensitivity was 22.1% for differentiating non-KD from KD patients. Clustering analysis identified three phenogroups that differed in a clinical, laboratory, and echocardiographic parameters. Compared with phenogroup I, phenogroup III had the highest prevalence of KD (91%), worse inflammatory markers, more deranged liver function, higher coronary artery <i>z</i> scores, and lower hematocrit and albumin levels. Abnormal blood parameters in febrile children with <i>z</i> scores of coronary artery segments <0.5 and 0.5-1.5 was associated with increased risks of having KD to 8.7 (<i>P</i> = 0.003) and 4.4 (<i>P</i> = 0.002), respectively.</p><p><strong>Interpretation: </strong>Phenomapping of febrile children with and without KD identified useful laboratory parameters that aid the diagnosis of KD in febrile children with relatively normal-sized coronary arteries.</p>","PeriodicalId":19992,"journal":{"name":"Pediatric Investigation","volume":"6 4","pages":"233-240"},"PeriodicalIF":2.0000,"publicationDate":"2022-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/3b/PED4-6-233.PMC9789931.pdf","citationCount":"0","resultStr":"{\"title\":\"Phenomapping approach to interpreting coronary dimensions in febrile children.\",\"authors\":\"Haoxun Tang, Xin Guo, Xiaolu Nie, Lin Zheng, Gang Liu, Wilfred Hing-Sang Wong, Yiu-Fai Cheung\",\"doi\":\"10.1002/ped4.12361\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Coronary artery dilation may occur in febrile children with and without Kawasaki disease (KD).</p><p><strong>Objective: </strong>We explored the application of unsupervised learning algorithms in the detection of novel patterns of coronary artery phenotypes in febrile children with and without KD.</p><p><strong>Methods: </strong>A total of 239 febrile children (59 non-KD and 180 KD patients), were recruited. Unsupervised hierarchical clustering analysis of phenotypic data including age, hemoglobin, white cell count, platelet count, C-reactive protein, erythrocyte sedimentation rate, albumin, alanine aminotransferase, aspartate aminotransferase, and coronary artery <i>z</i> scores were performed.</p><p><strong>Results: </strong>Using a cutoff <i>z</i> score of 2.5, the specificity was 98.3% and the sensitivity was 22.1% for differentiating non-KD from KD patients. Clustering analysis identified three phenogroups that differed in a clinical, laboratory, and echocardiographic parameters. Compared with phenogroup I, phenogroup III had the highest prevalence of KD (91%), worse inflammatory markers, more deranged liver function, higher coronary artery <i>z</i> scores, and lower hematocrit and albumin levels. Abnormal blood parameters in febrile children with <i>z</i> scores of coronary artery segments <0.5 and 0.5-1.5 was associated with increased risks of having KD to 8.7 (<i>P</i> = 0.003) and 4.4 (<i>P</i> = 0.002), respectively.</p><p><strong>Interpretation: </strong>Phenomapping of febrile children with and without KD identified useful laboratory parameters that aid the diagnosis of KD in febrile children with relatively normal-sized coronary arteries.</p>\",\"PeriodicalId\":19992,\"journal\":{\"name\":\"Pediatric Investigation\",\"volume\":\"6 4\",\"pages\":\"233-240\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2022-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/3b/PED4-6-233.PMC9789931.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ped4.12361\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ped4.12361","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
重要性:无论是否患有川崎病(KD),发热儿童都可能出现冠状动脉扩张:我们探索了无监督学习算法在检测发热儿童(无论是否患有川崎病)冠状动脉表型新模式中的应用:共招募了239名发热儿童(59名非KD患者和180名KD患者)。对年龄、血红蛋白、白细胞计数、血小板计数、C反应蛋白、红细胞沉降率、白蛋白、丙氨酸氨基转移酶、天门冬氨酸氨基转移酶和冠状动脉z评分等表型数据进行无监督分层聚类分析:以 Z 评分 2.5 为临界值,区分非 KD 和 KD 患者的特异性为 98.3%,敏感性为 22.1%。聚类分析确定了在临床、实验室和超声心动图参数方面存在差异的三个表型组。与表型组 I 相比,表型组 III 的 KD 患病率最高(91%)、炎症指标更差、肝功能更紊乱、冠状动脉 Z 评分更高、血细胞比容和白蛋白水平更低。发热儿童血液指标异常,冠状动脉分段z评分分别为P = 0.003)和4.4(P = 0.002):对患有和未患有 KD 的发热儿童进行表型分析,发现了一些有用的实验室指标,有助于对冠状动脉大小相对正常的发热儿童进行 KD 诊断。
Phenomapping approach to interpreting coronary dimensions in febrile children.
Importance: Coronary artery dilation may occur in febrile children with and without Kawasaki disease (KD).
Objective: We explored the application of unsupervised learning algorithms in the detection of novel patterns of coronary artery phenotypes in febrile children with and without KD.
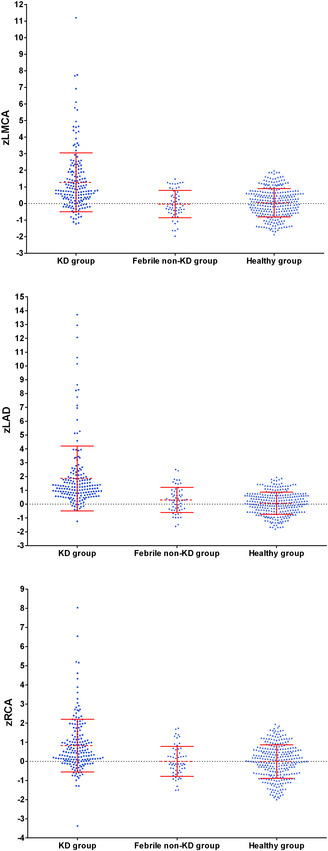
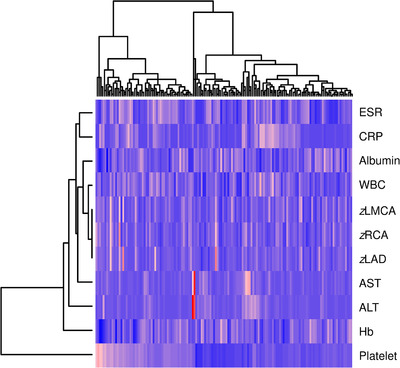
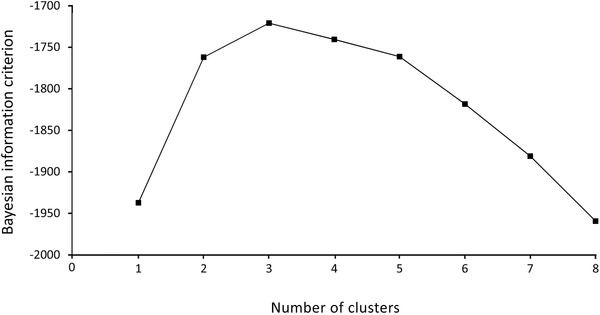
Methods: A total of 239 febrile children (59 non-KD and 180 KD patients), were recruited. Unsupervised hierarchical clustering analysis of phenotypic data including age, hemoglobin, white cell count, platelet count, C-reactive protein, erythrocyte sedimentation rate, albumin, alanine aminotransferase, aspartate aminotransferase, and coronary artery z scores were performed.
Results: Using a cutoff z score of 2.5, the specificity was 98.3% and the sensitivity was 22.1% for differentiating non-KD from KD patients. Clustering analysis identified three phenogroups that differed in a clinical, laboratory, and echocardiographic parameters. Compared with phenogroup I, phenogroup III had the highest prevalence of KD (91%), worse inflammatory markers, more deranged liver function, higher coronary artery z scores, and lower hematocrit and albumin levels. Abnormal blood parameters in febrile children with z scores of coronary artery segments <0.5 and 0.5-1.5 was associated with increased risks of having KD to 8.7 (P = 0.003) and 4.4 (P = 0.002), respectively.
Interpretation: Phenomapping of febrile children with and without KD identified useful laboratory parameters that aid the diagnosis of KD in febrile children with relatively normal-sized coronary arteries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
