Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang, Omar Galárraga
{"title":"支持家庭护理以预防东非孤儿和失散儿童中的艾滋病毒和死亡的成本效用:基于马尔可夫模型的模拟。","authors":"Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang, Omar Galárraga","doi":"10.1177/23814683221143782","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose.</b> Strengthening family-based care is a key policy response to the more than 15 million orphaned and separated children who have lost 1 or both parents in sub-Saharan Africa. This analysis estimated the cost-effectiveness of family-based care environments for preventing HIV and death in this population. <b>Design.</b> We developed a time-homogeneous Markov model to simulate the incremental cost per disability-adjusted life year (DALY) averted by supporting family-based environments caring for orphaned and separated children in western Kenya. Model parameters were based on data from the longitudinal OSCAR's Health and Well-Being Project and published literature. We used a societal perspective, annual cycle length, and 3% discount rate. Incremental cost-effectiveness ratios were simulated over 5- to 15-y horizons, comparing family-based settings to street-based \"self-care.\" Parameter uncertainty was addressed via deterministic and probabilistic sensitivity analyses. <b>Results.</b> Under base-case assumptions, family-based environments prevented 422 HIV infections and 298 deaths in a simulated cohort of 1,000 individuals over 10 y. Compared with street-based self-care, family-based care had an incremental cost of $2,528 per DALY averted (95% confidence interval [CI]: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413). The probability of family-based care being highly cost-effective was >80% at a willingness-to-pay (WTP) threshold of $2,250/DALY averted. Households receiving government cash transfers had minimally higher cost-effectiveness ratios than households without cash transfers but were still cost-effective at a WTP threshold of twice Kenya's GDP per capita. <b>Conclusions.</b> Compared with the status quo of street-based self-care, family-based environments offer a cost-effective approach for preventing HIV and death among orphaned children in lower-middle income countries. Decision makers should consider increasing resources to these environments in tandem with social protection programs.</p><p><strong>Highlights: </strong>UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world's most vulnerable children.This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.Compared with street-based \"self-care,\" family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"7 2","pages":"23814683221143782"},"PeriodicalIF":1.7000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/8a/10.1177_23814683221143782.PMC9806382.pdf","citationCount":"0","resultStr":"{\"title\":\"Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model-Based Simulation.\",\"authors\":\"Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang, Omar Galárraga\",\"doi\":\"10.1177/23814683221143782\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Purpose.</b> Strengthening family-based care is a key policy response to the more than 15 million orphaned and separated children who have lost 1 or both parents in sub-Saharan Africa. This analysis estimated the cost-effectiveness of family-based care environments for preventing HIV and death in this population. <b>Design.</b> We developed a time-homogeneous Markov model to simulate the incremental cost per disability-adjusted life year (DALY) averted by supporting family-based environments caring for orphaned and separated children in western Kenya. Model parameters were based on data from the longitudinal OSCAR's Health and Well-Being Project and published literature. We used a societal perspective, annual cycle length, and 3% discount rate. Incremental cost-effectiveness ratios were simulated over 5- to 15-y horizons, comparing family-based settings to street-based \\\"self-care.\\\" Parameter uncertainty was addressed via deterministic and probabilistic sensitivity analyses. <b>Results.</b> Under base-case assumptions, family-based environments prevented 422 HIV infections and 298 deaths in a simulated cohort of 1,000 individuals over 10 y. Compared with street-based self-care, family-based care had an incremental cost of $2,528 per DALY averted (95% confidence interval [CI]: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413). The probability of family-based care being highly cost-effective was >80% at a willingness-to-pay (WTP) threshold of $2,250/DALY averted. Households receiving government cash transfers had minimally higher cost-effectiveness ratios than households without cash transfers but were still cost-effective at a WTP threshold of twice Kenya's GDP per capita. <b>Conclusions.</b> Compared with the status quo of street-based self-care, family-based environments offer a cost-effective approach for preventing HIV and death among orphaned children in lower-middle income countries. Decision makers should consider increasing resources to these environments in tandem with social protection programs.</p><p><strong>Highlights: </strong>UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world's most vulnerable children.This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.Compared with street-based \\\"self-care,\\\" family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.</p>\",\"PeriodicalId\":36567,\"journal\":{\"name\":\"MDM Policy and Practice\",\"volume\":\"7 2\",\"pages\":\"23814683221143782\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/8a/10.1177_23814683221143782.PMC9806382.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MDM Policy and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23814683221143782\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683221143782","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model-Based Simulation.
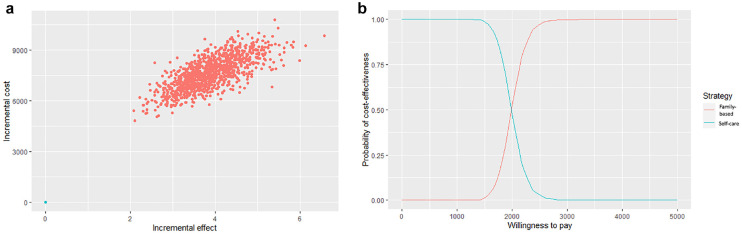
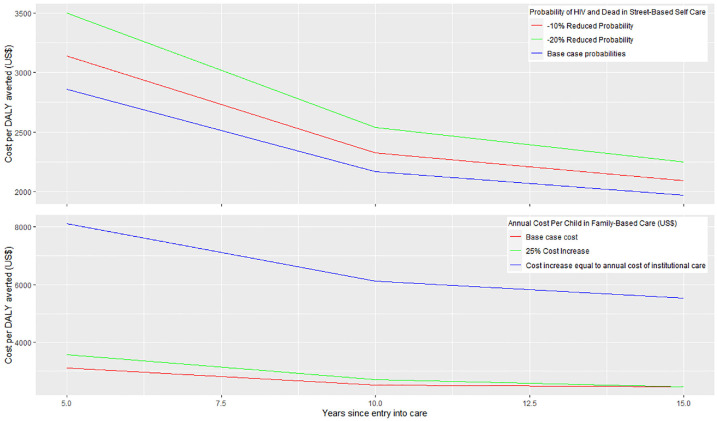
Purpose. Strengthening family-based care is a key policy response to the more than 15 million orphaned and separated children who have lost 1 or both parents in sub-Saharan Africa. This analysis estimated the cost-effectiveness of family-based care environments for preventing HIV and death in this population. Design. We developed a time-homogeneous Markov model to simulate the incremental cost per disability-adjusted life year (DALY) averted by supporting family-based environments caring for orphaned and separated children in western Kenya. Model parameters were based on data from the longitudinal OSCAR's Health and Well-Being Project and published literature. We used a societal perspective, annual cycle length, and 3% discount rate. Incremental cost-effectiveness ratios were simulated over 5- to 15-y horizons, comparing family-based settings to street-based "self-care." Parameter uncertainty was addressed via deterministic and probabilistic sensitivity analyses. Results. Under base-case assumptions, family-based environments prevented 422 HIV infections and 298 deaths in a simulated cohort of 1,000 individuals over 10 y. Compared with street-based self-care, family-based care had an incremental cost of $2,528 per DALY averted (95% confidence interval [CI]: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413). The probability of family-based care being highly cost-effective was >80% at a willingness-to-pay (WTP) threshold of $2,250/DALY averted. Households receiving government cash transfers had minimally higher cost-effectiveness ratios than households without cash transfers but were still cost-effective at a WTP threshold of twice Kenya's GDP per capita. Conclusions. Compared with the status quo of street-based self-care, family-based environments offer a cost-effective approach for preventing HIV and death among orphaned children in lower-middle income countries. Decision makers should consider increasing resources to these environments in tandem with social protection programs.
Highlights: UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world's most vulnerable children.This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.Compared with street-based "self-care," family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
