{"title":"在评估2019年美国冠状病毒病死亡率时应考虑院前心脏骤停。","authors":"Nick Williams","doi":"10.1055/a-2015-1244","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Public health emergencies leave little time to develop novel surveillance efforts. Understanding which preexisting clinical datasets are fit for surveillance use is of high value. Coronavirus disease 2019 (COVID-19) offers a natural applied informatics experiment to understand the fitness of clinical datasets for use in disease surveillance.</p><p><strong>Objectives: </strong>This study evaluates the agreement between legacy surveillance time series data and discovers their relative fitness for use in understanding the severity of the COVID-19 emergency. Here fitness for use means the statistical agreement between events across series.</p><p><strong>Methods: </strong>Thirteen weekly clinical event series from before and during the COVID-19 era for the United States were collected and integrated into a (multi) time series event data model. The Centers for Disease Control and Prevention (CDC) COVID-19 attributable mortality, CDC's excess mortality model, national Emergency Medical Services (EMS) calls, and Medicare encounter level claims were the data sources considered in this study. Cases were indexed by week from January 2015 through June of 2021 and fit to Distributed Random Forest models. Models returned the variable importance when predicting the series of interest from the remaining time series.</p><p><strong>Results: </strong>Model r2 statistics ranged from 0.78 to 0.99 for the share of the volumes predicted correctly. Prehospital data were of high value, and cardiac arrest (CA) prior to EMS arrival was on average the best predictor (tied with study week). COVID-19 Medicare claims volumes can predict COVID-19 death certificates (agreement), while viral respiratory Medicare claim volumes cannot predict Medicare COVID-19 claims (disagreement).</p><p><strong>Conclusion: </strong>Prehospital EMS data should be considered when evaluating the severity of COVID-19 because prehospital CA known to EMS was the strongest predictor on average across indices.</p>","PeriodicalId":49822,"journal":{"name":"Methods of Information in Medicine","volume":"62 3-04","pages":"100-109"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/24/10-1055-a-2015-1244.PMC10462431.pdf","citationCount":"0","resultStr":"{\"title\":\"Prehospital Cardiac Arrest Should be Considered When Evaluating Coronavirus Disease 2019 Mortality in the United States.\",\"authors\":\"Nick Williams\",\"doi\":\"10.1055/a-2015-1244\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Public health emergencies leave little time to develop novel surveillance efforts. Understanding which preexisting clinical datasets are fit for surveillance use is of high value. Coronavirus disease 2019 (COVID-19) offers a natural applied informatics experiment to understand the fitness of clinical datasets for use in disease surveillance.</p><p><strong>Objectives: </strong>This study evaluates the agreement between legacy surveillance time series data and discovers their relative fitness for use in understanding the severity of the COVID-19 emergency. Here fitness for use means the statistical agreement between events across series.</p><p><strong>Methods: </strong>Thirteen weekly clinical event series from before and during the COVID-19 era for the United States were collected and integrated into a (multi) time series event data model. The Centers for Disease Control and Prevention (CDC) COVID-19 attributable mortality, CDC's excess mortality model, national Emergency Medical Services (EMS) calls, and Medicare encounter level claims were the data sources considered in this study. Cases were indexed by week from January 2015 through June of 2021 and fit to Distributed Random Forest models. Models returned the variable importance when predicting the series of interest from the remaining time series.</p><p><strong>Results: </strong>Model r2 statistics ranged from 0.78 to 0.99 for the share of the volumes predicted correctly. Prehospital data were of high value, and cardiac arrest (CA) prior to EMS arrival was on average the best predictor (tied with study week). COVID-19 Medicare claims volumes can predict COVID-19 death certificates (agreement), while viral respiratory Medicare claim volumes cannot predict Medicare COVID-19 claims (disagreement).</p><p><strong>Conclusion: </strong>Prehospital EMS data should be considered when evaluating the severity of COVID-19 because prehospital CA known to EMS was the strongest predictor on average across indices.</p>\",\"PeriodicalId\":49822,\"journal\":{\"name\":\"Methods of Information in Medicine\",\"volume\":\"62 3-04\",\"pages\":\"100-109\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/24/10-1055-a-2015-1244.PMC10462431.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Methods of Information in Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2015-1244\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"COMPUTER SCIENCE, INFORMATION SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Methods of Information in Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2015-1244","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"COMPUTER SCIENCE, INFORMATION SYSTEMS","Score":null,"Total":0}
Prehospital Cardiac Arrest Should be Considered When Evaluating Coronavirus Disease 2019 Mortality in the United States.
Background: Public health emergencies leave little time to develop novel surveillance efforts. Understanding which preexisting clinical datasets are fit for surveillance use is of high value. Coronavirus disease 2019 (COVID-19) offers a natural applied informatics experiment to understand the fitness of clinical datasets for use in disease surveillance.
Objectives: This study evaluates the agreement between legacy surveillance time series data and discovers their relative fitness for use in understanding the severity of the COVID-19 emergency. Here fitness for use means the statistical agreement between events across series.
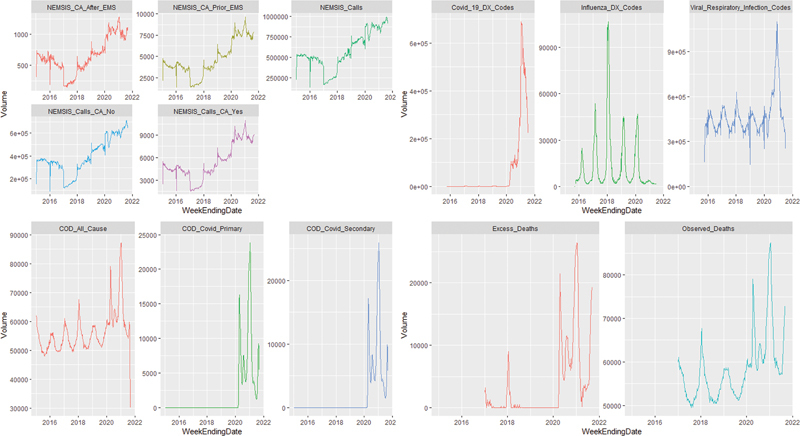
Methods: Thirteen weekly clinical event series from before and during the COVID-19 era for the United States were collected and integrated into a (multi) time series event data model. The Centers for Disease Control and Prevention (CDC) COVID-19 attributable mortality, CDC's excess mortality model, national Emergency Medical Services (EMS) calls, and Medicare encounter level claims were the data sources considered in this study. Cases were indexed by week from January 2015 through June of 2021 and fit to Distributed Random Forest models. Models returned the variable importance when predicting the series of interest from the remaining time series.
Results: Model r2 statistics ranged from 0.78 to 0.99 for the share of the volumes predicted correctly. Prehospital data were of high value, and cardiac arrest (CA) prior to EMS arrival was on average the best predictor (tied with study week). COVID-19 Medicare claims volumes can predict COVID-19 death certificates (agreement), while viral respiratory Medicare claim volumes cannot predict Medicare COVID-19 claims (disagreement).
Conclusion: Prehospital EMS data should be considered when evaluating the severity of COVID-19 because prehospital CA known to EMS was the strongest predictor on average across indices.
期刊介绍:
Good medicine and good healthcare demand good information. Since the journal''s founding in 1962, Methods of Information in Medicine has stressed the methodology and scientific fundamentals of organizing, representing and analyzing data, information and knowledge in biomedicine and health care. Covering publications in the fields of biomedical and health informatics, medical biometry, and epidemiology, the journal publishes original papers, reviews, reports, opinion papers, editorials, and letters to the editor. From time to time, the journal publishes articles on particular focus themes as part of a journal''s issue.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
