{"title":"在介入性疼痛管理中不再有手术部位感染引起的撕裂。","authors":"Seungjin Lim, Yeong-Min Yoo, Kyung-Hoon Kim","doi":"10.3344/kjp.22397","DOIUrl":null,"url":null,"abstract":"<p><p>As the field of interventional pain management (IPM) grows, the risk of surgical site infections (SSIs) is increasing. SSI is defined as an infection of the incision or organ/space that occurs within one month after operation or three months after implantation. It is also common to find patients with suspected infection in an outpatient clinic. The most frequent IPM procedures are performed in the spine. Even though primary pyogenic spondylodiscitis <i>via</i> hematogenous spread is the most common type among spinal infections, secondary spinal infections from direct inoculation should be monitored after IPM procedures. Various preventive guidelines for SSI have been published. Cefazolin, followed by vancomycin, is the most commonly used surgical antibiotic prophylaxis in IPM. Diagnosis of SSI is confirmed by purulent discharge, isolation of causative organisms, pain/tenderness, swelling, redness, or heat, or diagnosis by a surgeon or attending physician. Inflammatory markers include traditional (C-reactive protein, erythrocyte sedimentation rate, and white blood cell count) and novel (procalcitonin, serum amyloid A, and presepsin) markers. Empirical antibiotic therapy is defined as the initial administration of antibiotics within at least 24 hours prior to the results of blood culture and antibiotic susceptibility testing. Definitive antibiotic therapy is initiated based on the above culture and testing. Combination antibiotic therapy for multidrug-resistant Gram-negative bacteria infections appears to be superior to monotherapy in mortality with the risk of increasing antibiotic resistance rates. The never-ending war between bacterial resistance and new antibiotics is continuing. This article reviews prevention, diagnosis, and treatment of infection in pain medicine.</p>","PeriodicalId":56252,"journal":{"name":"Korean Journal of Pain","volume":"36 1","pages":"11-50"},"PeriodicalIF":3.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/dc/kjp-36-1-11.PMC9812697.pdf","citationCount":"1","resultStr":"{\"title\":\"No more tears from surgical site infections in interventional pain management.\",\"authors\":\"Seungjin Lim, Yeong-Min Yoo, Kyung-Hoon Kim\",\"doi\":\"10.3344/kjp.22397\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>As the field of interventional pain management (IPM) grows, the risk of surgical site infections (SSIs) is increasing. SSI is defined as an infection of the incision or organ/space that occurs within one month after operation or three months after implantation. It is also common to find patients with suspected infection in an outpatient clinic. The most frequent IPM procedures are performed in the spine. Even though primary pyogenic spondylodiscitis <i>via</i> hematogenous spread is the most common type among spinal infections, secondary spinal infections from direct inoculation should be monitored after IPM procedures. Various preventive guidelines for SSI have been published. Cefazolin, followed by vancomycin, is the most commonly used surgical antibiotic prophylaxis in IPM. Diagnosis of SSI is confirmed by purulent discharge, isolation of causative organisms, pain/tenderness, swelling, redness, or heat, or diagnosis by a surgeon or attending physician. Inflammatory markers include traditional (C-reactive protein, erythrocyte sedimentation rate, and white blood cell count) and novel (procalcitonin, serum amyloid A, and presepsin) markers. Empirical antibiotic therapy is defined as the initial administration of antibiotics within at least 24 hours prior to the results of blood culture and antibiotic susceptibility testing. Definitive antibiotic therapy is initiated based on the above culture and testing. Combination antibiotic therapy for multidrug-resistant Gram-negative bacteria infections appears to be superior to monotherapy in mortality with the risk of increasing antibiotic resistance rates. The never-ending war between bacterial resistance and new antibiotics is continuing. This article reviews prevention, diagnosis, and treatment of infection in pain medicine.</p>\",\"PeriodicalId\":56252,\"journal\":{\"name\":\"Korean Journal of Pain\",\"volume\":\"36 1\",\"pages\":\"11-50\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/dc/kjp-36-1-11.PMC9812697.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Pain\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3344/kjp.22397\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Pain","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3344/kjp.22397","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
No more tears from surgical site infections in interventional pain management.
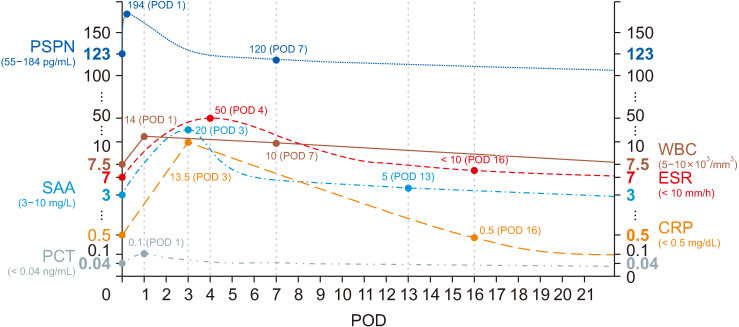
As the field of interventional pain management (IPM) grows, the risk of surgical site infections (SSIs) is increasing. SSI is defined as an infection of the incision or organ/space that occurs within one month after operation or three months after implantation. It is also common to find patients with suspected infection in an outpatient clinic. The most frequent IPM procedures are performed in the spine. Even though primary pyogenic spondylodiscitis via hematogenous spread is the most common type among spinal infections, secondary spinal infections from direct inoculation should be monitored after IPM procedures. Various preventive guidelines for SSI have been published. Cefazolin, followed by vancomycin, is the most commonly used surgical antibiotic prophylaxis in IPM. Diagnosis of SSI is confirmed by purulent discharge, isolation of causative organisms, pain/tenderness, swelling, redness, or heat, or diagnosis by a surgeon or attending physician. Inflammatory markers include traditional (C-reactive protein, erythrocyte sedimentation rate, and white blood cell count) and novel (procalcitonin, serum amyloid A, and presepsin) markers. Empirical antibiotic therapy is defined as the initial administration of antibiotics within at least 24 hours prior to the results of blood culture and antibiotic susceptibility testing. Definitive antibiotic therapy is initiated based on the above culture and testing. Combination antibiotic therapy for multidrug-resistant Gram-negative bacteria infections appears to be superior to monotherapy in mortality with the risk of increasing antibiotic resistance rates. The never-ending war between bacterial resistance and new antibiotics is continuing. This article reviews prevention, diagnosis, and treatment of infection in pain medicine.
期刊介绍:
Korean Journal of Pain (Korean J Pain, KJP) is the official journal of the Korean Pain Society, founded in 1986. It has been published since 1988. It publishes peer reviewed original articles related to all aspects of pain, including clinical and basic research, patient care, education, and health policy. It has been published quarterly in English since 2009 (on the first day of January, April, July, and October). In addition, it has also become the official journal of the International Spinal Pain Society since 2016. The mission of the Journal is to improve the care of patients in pain by providing a forum for clinical researchers, basic scientists, clinicians, and other health professionals. The circulation number per issue is 50.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
