Jun Yeong Song, Eui Kyu Chie, Seong-Hee Kang, Yeon-Jun Jeon, Yoon-Ah Ko, Dong-Yun Kim, Hyun-Cheol Kang
{"title":"磁共振成像引导下胰腺癌适应性放射治疗的剂量学评价:危险器官再轮廓的程度。","authors":"Jun Yeong Song, Eui Kyu Chie, Seong-Hee Kang, Yeon-Jun Jeon, Yoon-Ah Ko, Dong-Yun Kim, Hyun-Cheol Kang","doi":"10.3857/roj.2022.00332","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The safety of online contouring and planning for adaptive radiotherapy is unknown. This study aimed to evaluate the dosimetric difference of the organ-at-risk (OAR) according to the extent of contouring in stereotactic magnetic resonance image-guided adaptive RT (SMART) for pancreatic cancer.</p><p><strong>Materials and methods: </strong>We reviewed the treatment plan data used for SMART in patients with pancreatic cancer. For the online contouring and planning, OARs within 2 cm from the planning target volume (PTV) in the craniocaudal direction were re-controlled daily at the attending physician's discretion. The entire OARs were re-contoured retrospectively for data analysis. We termed the two contouring methods the Rough OAR and the Full OAR, respectively. The proportion of dose constraint violation and other dosimetric parameters was analyzed.</p><p><strong>Results: </strong>Nineteen patients with 94 fractions of SMART were included in the analysis. The dose constraint was violated in 10.6% and 43.6% of the fractions in Rough OAR and Full OAR methods, respectively (p = 0.075). Patients with a large tumor, a short distance from gross tumor volume (GTV) to OAR, and a tumor in the body or tail were associated with more occult dose constraint violations-large tumor (p = 0.027), short distance from GTV to OAR (p = 0.061), tumor in body or tail (p = 0.054). No dose constraint violation occurred outside 2 cm from the PTV.</p><p><strong>Conclusion: </strong>More occult dose constraint violations can be found by the Full OAR method in patients with pancreatic cancer with some clinical factors in the online re-planning for SMART. Re-contouring all the OARs would be helpful to detect occult dose constraint violations in SMART planning. Since the dosimetric profile of SMART cannot be represented by a single fraction, patient selection for the Full OAR method should be weighted between the clinical usefulness and the time and workforce required.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"40 4","pages":"242-250"},"PeriodicalIF":2.2000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/d0/roj-2022-00332.PMC9830039.pdf","citationCount":"1","resultStr":"{\"title\":\"Dosimetric evaluation of magnetic resonance imaging-guided adaptive radiation therapy in pancreatic cancer by extent of re-contouring of organs-at-risk.\",\"authors\":\"Jun Yeong Song, Eui Kyu Chie, Seong-Hee Kang, Yeon-Jun Jeon, Yoon-Ah Ko, Dong-Yun Kim, Hyun-Cheol Kang\",\"doi\":\"10.3857/roj.2022.00332\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The safety of online contouring and planning for adaptive radiotherapy is unknown. This study aimed to evaluate the dosimetric difference of the organ-at-risk (OAR) according to the extent of contouring in stereotactic magnetic resonance image-guided adaptive RT (SMART) for pancreatic cancer.</p><p><strong>Materials and methods: </strong>We reviewed the treatment plan data used for SMART in patients with pancreatic cancer. For the online contouring and planning, OARs within 2 cm from the planning target volume (PTV) in the craniocaudal direction were re-controlled daily at the attending physician's discretion. The entire OARs were re-contoured retrospectively for data analysis. We termed the two contouring methods the Rough OAR and the Full OAR, respectively. The proportion of dose constraint violation and other dosimetric parameters was analyzed.</p><p><strong>Results: </strong>Nineteen patients with 94 fractions of SMART were included in the analysis. The dose constraint was violated in 10.6% and 43.6% of the fractions in Rough OAR and Full OAR methods, respectively (p = 0.075). Patients with a large tumor, a short distance from gross tumor volume (GTV) to OAR, and a tumor in the body or tail were associated with more occult dose constraint violations-large tumor (p = 0.027), short distance from GTV to OAR (p = 0.061), tumor in body or tail (p = 0.054). No dose constraint violation occurred outside 2 cm from the PTV.</p><p><strong>Conclusion: </strong>More occult dose constraint violations can be found by the Full OAR method in patients with pancreatic cancer with some clinical factors in the online re-planning for SMART. Re-contouring all the OARs would be helpful to detect occult dose constraint violations in SMART planning. Since the dosimetric profile of SMART cannot be represented by a single fraction, patient selection for the Full OAR method should be weighted between the clinical usefulness and the time and workforce required.</p>\",\"PeriodicalId\":46572,\"journal\":{\"name\":\"Radiation Oncology Journal\",\"volume\":\"40 4\",\"pages\":\"242-250\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/d0/roj-2022-00332.PMC9830039.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3857/roj.2022.00332\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2022.00332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Dosimetric evaluation of magnetic resonance imaging-guided adaptive radiation therapy in pancreatic cancer by extent of re-contouring of organs-at-risk.
Purpose: The safety of online contouring and planning for adaptive radiotherapy is unknown. This study aimed to evaluate the dosimetric difference of the organ-at-risk (OAR) according to the extent of contouring in stereotactic magnetic resonance image-guided adaptive RT (SMART) for pancreatic cancer.
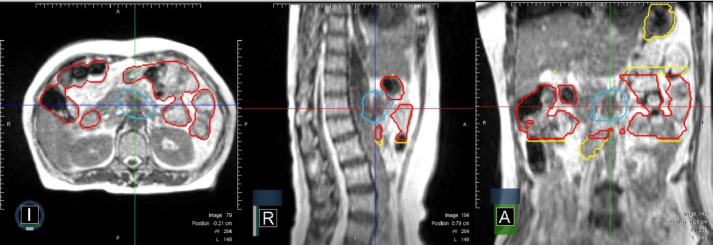
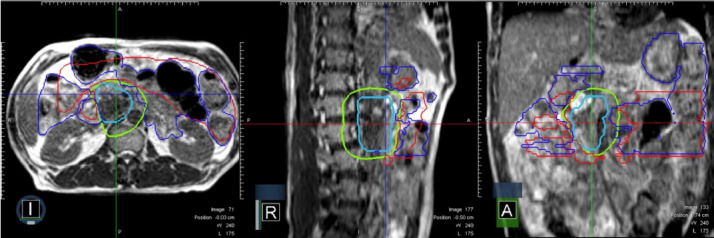
Materials and methods: We reviewed the treatment plan data used for SMART in patients with pancreatic cancer. For the online contouring and planning, OARs within 2 cm from the planning target volume (PTV) in the craniocaudal direction were re-controlled daily at the attending physician's discretion. The entire OARs were re-contoured retrospectively for data analysis. We termed the two contouring methods the Rough OAR and the Full OAR, respectively. The proportion of dose constraint violation and other dosimetric parameters was analyzed.
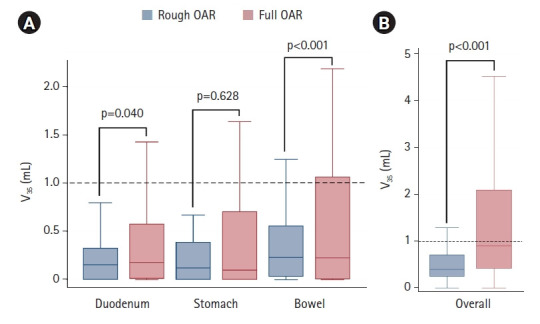
Results: Nineteen patients with 94 fractions of SMART were included in the analysis. The dose constraint was violated in 10.6% and 43.6% of the fractions in Rough OAR and Full OAR methods, respectively (p = 0.075). Patients with a large tumor, a short distance from gross tumor volume (GTV) to OAR, and a tumor in the body or tail were associated with more occult dose constraint violations-large tumor (p = 0.027), short distance from GTV to OAR (p = 0.061), tumor in body or tail (p = 0.054). No dose constraint violation occurred outside 2 cm from the PTV.
Conclusion: More occult dose constraint violations can be found by the Full OAR method in patients with pancreatic cancer with some clinical factors in the online re-planning for SMART. Re-contouring all the OARs would be helpful to detect occult dose constraint violations in SMART planning. Since the dosimetric profile of SMART cannot be represented by a single fraction, patient selection for the Full OAR method should be weighted between the clinical usefulness and the time and workforce required.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
