David Ambinder, Shu Wang, Mohummad Minhaj Siddiqui
{"title":"确定机器人辅助根治性前列腺切除术中基于组件的手术时间学习曲线。","authors":"David Ambinder, Shu Wang, Mohummad Minhaj Siddiqui","doi":"10.1097/CU9.0000000000000119","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To determine the learning curve (LC) of total operative time and the discrete components of the robotic-assisted radical prostatectomy (RARP) for a recent robotic fellowship-trained urologic surgeon.</p><p><strong>Materials and methods: </strong>We performed a retrospective analysis of RARP procedures performed by a single new attending surgeon from August 2015 to April 2019. Patients' demographics and operative details were assessed. Total operative time was divided and prospectively recorded in 7 parts: (<i>a</i>) docking robot, (<i>b</i>) dissecting seminal vesicles (SVs) (<i>c</i>) dissecting endopelvic fascia (EPF), (<i>d</i>) incising bladder neck (BN), (<i>e</i>) completing the dissection, (<i>f</i>) lymph node dissection, and (<i>g</i>) urethrovesical anastomosis (UVA) and robot undocking. Cumulative sum analysis was used to ascertain the LC for total operative time and the 7 parts of the procedure.</p><p><strong>Results: </strong>One hundred twenty consecutive RARPs were performed. The LC was overcome at 25 cases for total operative time, 13 cases for docking the robot, 33 cases for dissecting SVs, 31 cases for dissecting EPF, 46 cases for incising BN, 38 cases for prostate dissection, 25 cases for lymph node dissection, and 52 cases for UVA. Total operative time was decreased 22.8% (<i>p</i> < 0.0001) and time for robot docking, dissecting SVs, dissecting EPF, incising BN, completing prostate dissection, lymph node dissection, and UVA were decreased 16.7%, 30.5%, 29.5%, 36.2%, 37.3%, 32.2%, and 26.9%, respectively (all <i>p</i> < 0.05).</p><p><strong>Conclusions: </strong>We observed a 25-case LC for a fellowship-trained urologist to achieve stable operative performance of RARP surgery. Procedural components demonstrated variable LCs including the UVA that required upward of 52 cases.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"16 4","pages":"240-245"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ba/7a/curr-urol-16-240.PMC9875207.pdf","citationCount":"0","resultStr":"{\"title\":\"Determining the component-based operative time learning curve for robotic-assisted radical prostatectomy.\",\"authors\":\"David Ambinder, Shu Wang, Mohummad Minhaj Siddiqui\",\"doi\":\"10.1097/CU9.0000000000000119\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To determine the learning curve (LC) of total operative time and the discrete components of the robotic-assisted radical prostatectomy (RARP) for a recent robotic fellowship-trained urologic surgeon.</p><p><strong>Materials and methods: </strong>We performed a retrospective analysis of RARP procedures performed by a single new attending surgeon from August 2015 to April 2019. Patients' demographics and operative details were assessed. Total operative time was divided and prospectively recorded in 7 parts: (<i>a</i>) docking robot, (<i>b</i>) dissecting seminal vesicles (SVs) (<i>c</i>) dissecting endopelvic fascia (EPF), (<i>d</i>) incising bladder neck (BN), (<i>e</i>) completing the dissection, (<i>f</i>) lymph node dissection, and (<i>g</i>) urethrovesical anastomosis (UVA) and robot undocking. Cumulative sum analysis was used to ascertain the LC for total operative time and the 7 parts of the procedure.</p><p><strong>Results: </strong>One hundred twenty consecutive RARPs were performed. The LC was overcome at 25 cases for total operative time, 13 cases for docking the robot, 33 cases for dissecting SVs, 31 cases for dissecting EPF, 46 cases for incising BN, 38 cases for prostate dissection, 25 cases for lymph node dissection, and 52 cases for UVA. Total operative time was decreased 22.8% (<i>p</i> < 0.0001) and time for robot docking, dissecting SVs, dissecting EPF, incising BN, completing prostate dissection, lymph node dissection, and UVA were decreased 16.7%, 30.5%, 29.5%, 36.2%, 37.3%, 32.2%, and 26.9%, respectively (all <i>p</i> < 0.05).</p><p><strong>Conclusions: </strong>We observed a 25-case LC for a fellowship-trained urologist to achieve stable operative performance of RARP surgery. Procedural components demonstrated variable LCs including the UVA that required upward of 52 cases.</p>\",\"PeriodicalId\":39147,\"journal\":{\"name\":\"Current Urology\",\"volume\":\"16 4\",\"pages\":\"240-245\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ba/7a/curr-urol-16-240.PMC9875207.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CU9.0000000000000119\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000119","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Determining the component-based operative time learning curve for robotic-assisted radical prostatectomy.
Objectives: To determine the learning curve (LC) of total operative time and the discrete components of the robotic-assisted radical prostatectomy (RARP) for a recent robotic fellowship-trained urologic surgeon.
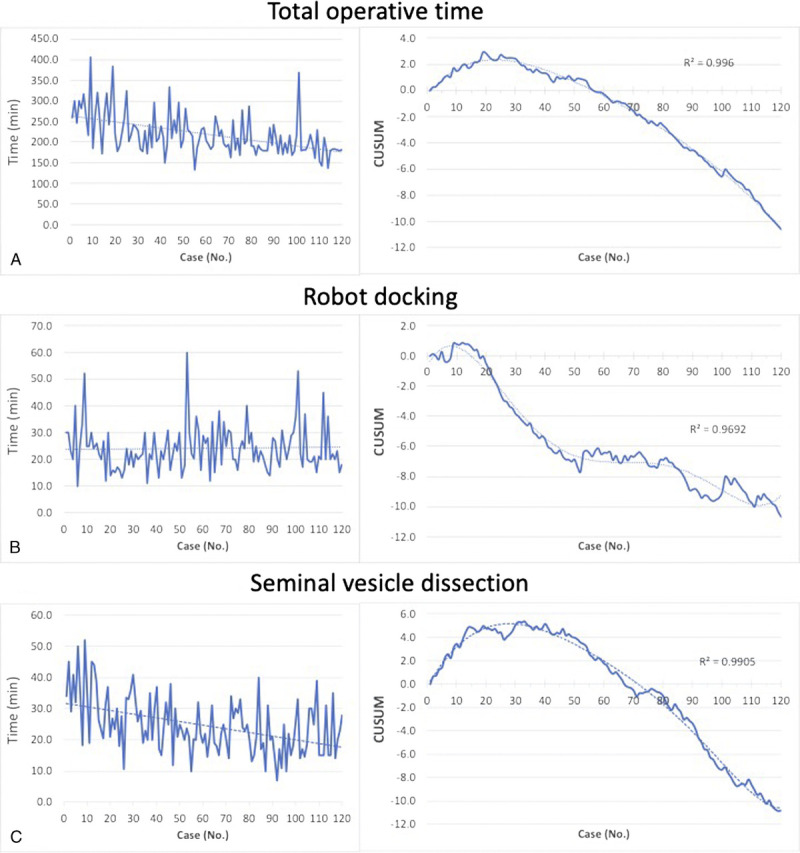
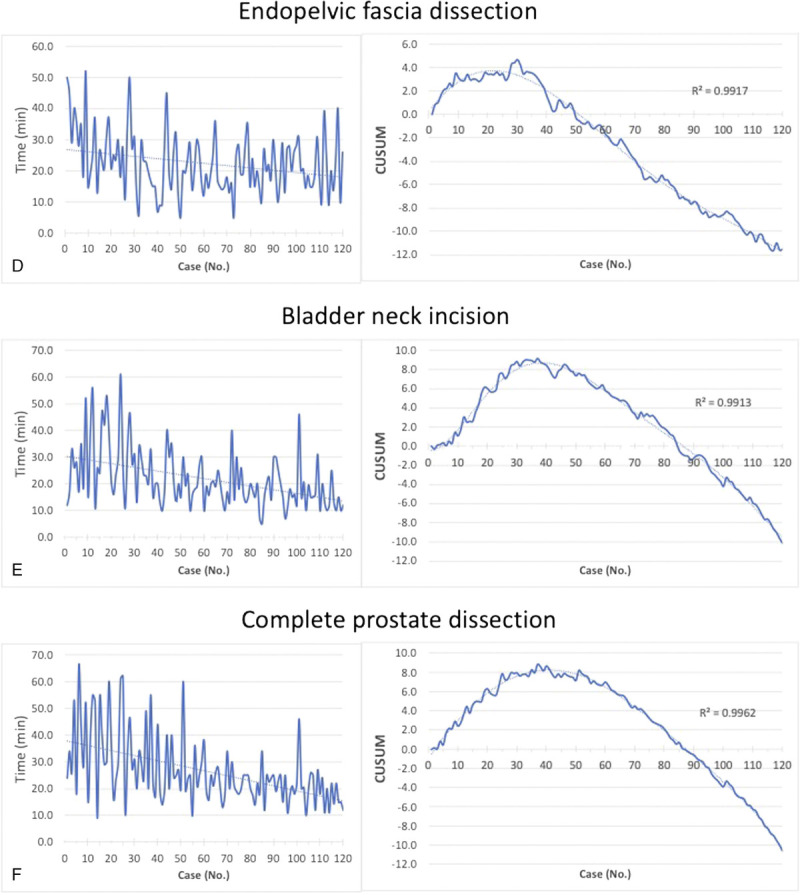
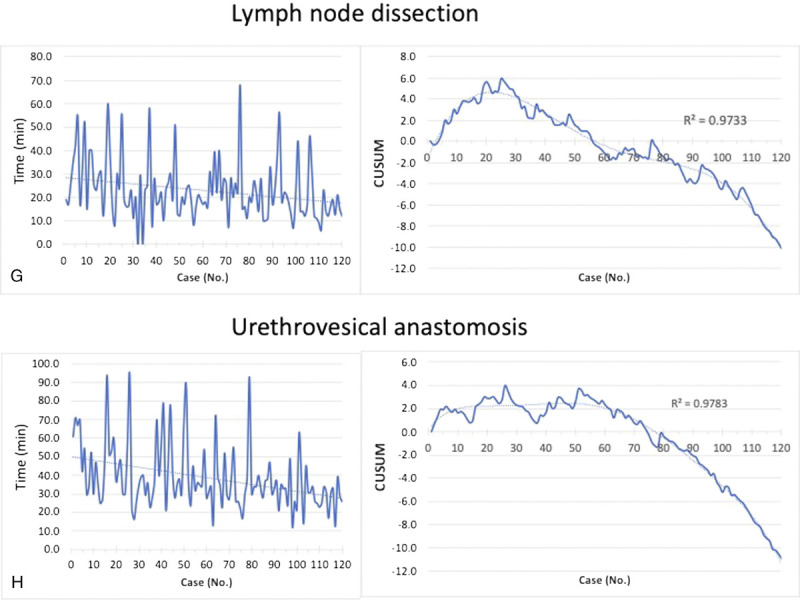
Materials and methods: We performed a retrospective analysis of RARP procedures performed by a single new attending surgeon from August 2015 to April 2019. Patients' demographics and operative details were assessed. Total operative time was divided and prospectively recorded in 7 parts: (a) docking robot, (b) dissecting seminal vesicles (SVs) (c) dissecting endopelvic fascia (EPF), (d) incising bladder neck (BN), (e) completing the dissection, (f) lymph node dissection, and (g) urethrovesical anastomosis (UVA) and robot undocking. Cumulative sum analysis was used to ascertain the LC for total operative time and the 7 parts of the procedure.
Results: One hundred twenty consecutive RARPs were performed. The LC was overcome at 25 cases for total operative time, 13 cases for docking the robot, 33 cases for dissecting SVs, 31 cases for dissecting EPF, 46 cases for incising BN, 38 cases for prostate dissection, 25 cases for lymph node dissection, and 52 cases for UVA. Total operative time was decreased 22.8% (p < 0.0001) and time for robot docking, dissecting SVs, dissecting EPF, incising BN, completing prostate dissection, lymph node dissection, and UVA were decreased 16.7%, 30.5%, 29.5%, 36.2%, 37.3%, 32.2%, and 26.9%, respectively (all p < 0.05).
Conclusions: We observed a 25-case LC for a fellowship-trained urologist to achieve stable operative performance of RARP surgery. Procedural components demonstrated variable LCs including the UVA that required upward of 52 cases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
