Philippe Wibart, Thomas Réginault, Margarita Garcia-Fontan, Bérangère Barbrel, Clement Bader, Antoine Benard, Verônica Franco Parreira, Daniel Gonzalez-Antón, Nam H Bui, Didier Gruson, Gilles Hilbert, Roberto Martinez-Alejos, Frédéric Vargas
{"title":"机械通气在预防重症监护获得性虚弱患者拔管后急性呼吸衰竭中的作用:一项随机对照试验。","authors":"Philippe Wibart, Thomas Réginault, Margarita Garcia-Fontan, Bérangère Barbrel, Clement Bader, Antoine Benard, Verônica Franco Parreira, Daniel Gonzalez-Antón, Nam H Bui, Didier Gruson, Gilles Hilbert, Roberto Martinez-Alejos, Frédéric Vargas","doi":"10.5935/2965-2774.20230410-en","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We hypothesized that the use of mechanical insufflation-exsufflation can reduce the incidence of acute respiratory failure within the 48-hour post-extubation period in intensive care unit-acquired weakness patients.</p><p><strong>Methods: </strong>This was a prospective randomized controlled open-label trial. Patients diagnosed with intensive care unit-acquired weakness were consecutively enrolled based on a Medical Research Council score ≤ 48/60. The patients randomly received two daily sessions; in the control group, conventional chest physiotherapy was performed, while in the intervention group, chest physiotherapy was associated with mechanical insufflation-exsufflation. The incidence of acute respiratory failure within 48 hours of extubation was evaluated. Similarly, the reintubation rate, intensive care unit length of stay, mortality at 28 days, and survival probability at 90 days were assessed. The study was stopped after futility results in the interim analysis.</p><p><strong>Results: </strong>We included 122 consecutive patients (n = 61 per group). There was no significant difference in the incidence of acute respiratory failure between treatments (11.5% control group versus 16.4%, intervention group; p = 0.60), the need for reintubation (3.6% versus 10.7%; p = 0.27), mean length of stay (3 versus 4 days; p = 0.33), mortality at Day 28 (9.8% versus 15.0%; p = 0.42), or survival probability at Day 90 (21.3% versus 28.3%; p = 0.41).</p><p><strong>Conclusion: </strong>Mechanical insufflation-exsufflation combined with chest physiotherapy seems to have no impact in preventing postextubation acute respiratory failure in intensive care unit-acquired weakness patients. Similarly, mortality and survival probability were similar in both groups. Nevertheless, given the early termination of the trial, further clinical investigation is strongly recommended.</p><p><strong>Clinical trials register: </strong>NCT01931228.</p>","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"35 2","pages":"168-176"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10406413/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of mechanical in-exsufflation in preventing postextubation acute respiratory failure in intensive care acquired weakness patients: a randomized controlled trial.\",\"authors\":\"Philippe Wibart, Thomas Réginault, Margarita Garcia-Fontan, Bérangère Barbrel, Clement Bader, Antoine Benard, Verônica Franco Parreira, Daniel Gonzalez-Antón, Nam H Bui, Didier Gruson, Gilles Hilbert, Roberto Martinez-Alejos, Frédéric Vargas\",\"doi\":\"10.5935/2965-2774.20230410-en\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We hypothesized that the use of mechanical insufflation-exsufflation can reduce the incidence of acute respiratory failure within the 48-hour post-extubation period in intensive care unit-acquired weakness patients.</p><p><strong>Methods: </strong>This was a prospective randomized controlled open-label trial. Patients diagnosed with intensive care unit-acquired weakness were consecutively enrolled based on a Medical Research Council score ≤ 48/60. The patients randomly received two daily sessions; in the control group, conventional chest physiotherapy was performed, while in the intervention group, chest physiotherapy was associated with mechanical insufflation-exsufflation. The incidence of acute respiratory failure within 48 hours of extubation was evaluated. Similarly, the reintubation rate, intensive care unit length of stay, mortality at 28 days, and survival probability at 90 days were assessed. The study was stopped after futility results in the interim analysis.</p><p><strong>Results: </strong>We included 122 consecutive patients (n = 61 per group). There was no significant difference in the incidence of acute respiratory failure between treatments (11.5% control group versus 16.4%, intervention group; p = 0.60), the need for reintubation (3.6% versus 10.7%; p = 0.27), mean length of stay (3 versus 4 days; p = 0.33), mortality at Day 28 (9.8% versus 15.0%; p = 0.42), or survival probability at Day 90 (21.3% versus 28.3%; p = 0.41).</p><p><strong>Conclusion: </strong>Mechanical insufflation-exsufflation combined with chest physiotherapy seems to have no impact in preventing postextubation acute respiratory failure in intensive care unit-acquired weakness patients. Similarly, mortality and survival probability were similar in both groups. Nevertheless, given the early termination of the trial, further clinical investigation is strongly recommended.</p><p><strong>Clinical trials register: </strong>NCT01931228.</p>\",\"PeriodicalId\":72721,\"journal\":{\"name\":\"Critical care science\",\"volume\":\"35 2\",\"pages\":\"168-176\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10406413/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5935/2965-2774.20230410-en\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5935/2965-2774.20230410-en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Effects of mechanical in-exsufflation in preventing postextubation acute respiratory failure in intensive care acquired weakness patients: a randomized controlled trial.
Objective: We hypothesized that the use of mechanical insufflation-exsufflation can reduce the incidence of acute respiratory failure within the 48-hour post-extubation period in intensive care unit-acquired weakness patients.
Methods: This was a prospective randomized controlled open-label trial. Patients diagnosed with intensive care unit-acquired weakness were consecutively enrolled based on a Medical Research Council score ≤ 48/60. The patients randomly received two daily sessions; in the control group, conventional chest physiotherapy was performed, while in the intervention group, chest physiotherapy was associated with mechanical insufflation-exsufflation. The incidence of acute respiratory failure within 48 hours of extubation was evaluated. Similarly, the reintubation rate, intensive care unit length of stay, mortality at 28 days, and survival probability at 90 days were assessed. The study was stopped after futility results in the interim analysis.
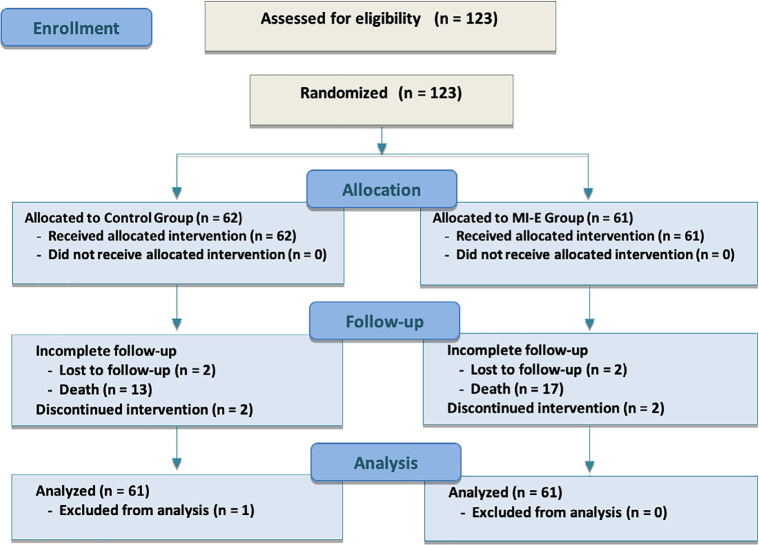
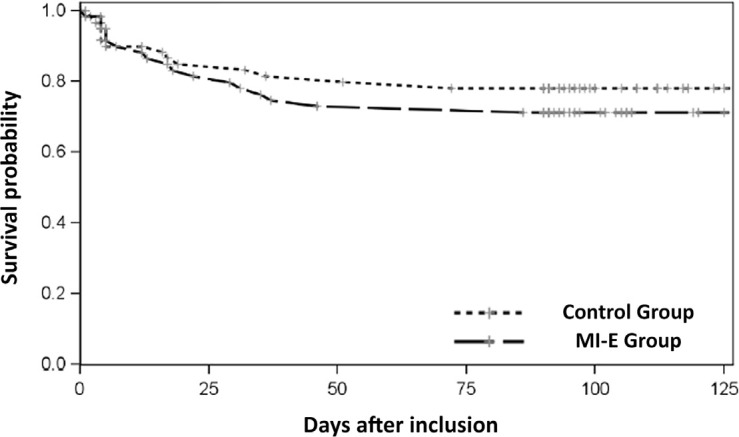
Results: We included 122 consecutive patients (n = 61 per group). There was no significant difference in the incidence of acute respiratory failure between treatments (11.5% control group versus 16.4%, intervention group; p = 0.60), the need for reintubation (3.6% versus 10.7%; p = 0.27), mean length of stay (3 versus 4 days; p = 0.33), mortality at Day 28 (9.8% versus 15.0%; p = 0.42), or survival probability at Day 90 (21.3% versus 28.3%; p = 0.41).
Conclusion: Mechanical insufflation-exsufflation combined with chest physiotherapy seems to have no impact in preventing postextubation acute respiratory failure in intensive care unit-acquired weakness patients. Similarly, mortality and survival probability were similar in both groups. Nevertheless, given the early termination of the trial, further clinical investigation is strongly recommended.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
