Efraín Farías-Cisneros, Jorge Luis Martínez-Peniche, Luis Carlos Olguín-Delgado, Francisco Guillermo Castillo-Vázquez, Ranulfo Romo-Rodríguez, Armando Torres-Gómez
{"title":"全肘关节置换术和顺行后骨间皮瓣治疗感染性创伤后关节炎伴活动瘘。综合治疗的基本原理。病例报告。","authors":"Efraín Farías-Cisneros, Jorge Luis Martínez-Peniche, Luis Carlos Olguín-Delgado, Francisco Guillermo Castillo-Vázquez, Ranulfo Romo-Rodríguez, Armando Torres-Gómez","doi":"10.1177/24715492221090745","DOIUrl":null,"url":null,"abstract":"<p><p>The indication for total elbow arthroplasty (TEA) for primary and posttraumatic elbow arthritis has increased, however, its indication after infection remains elusive. Wound closure about the elbow increases the challenge of treating a previously infected elbow, often necessitating soft tissue coverage with local or regional flaps. We present a 75-year-old male patient with an elbow infection following a failed complex intraarticular fracture open reduction and internal fixation of the distal humerus. Initially, he presented with severe functional impairment and pain, also with an active fistula with serous exudate, whose culture was positive for <i>Cutinebacterium acnes</i>. Septic hardware loosening, and septic nonunion with intraarticular involvement of the left elbow was diagnosed. The patient underwent hardware removal, fistulectomy, serial irrigation and debridement and a pedicled antegrade posterior interosseous artery (PIA) flap on staged surgical treatment. Finally, after ruling out infection persistence, a TEA was performed. We aim to report the outcome of a patient treated with a TEA in the context of a previously infected elbow with soft tissue coverage with an antegrade PIA flap. Comprehensive treatment must be done in an appropriate manner, to obtain an expedited and desirable outcome.</p>","PeriodicalId":73942,"journal":{"name":"Journal of shoulder and elbow arthroplasty","volume":"6 ","pages":"24715492221090745"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/a9/10.1177_24715492221090745.PMC9163731.pdf","citationCount":"0","resultStr":"{\"title\":\"Total Elbow Arthroplasty and Antegrade Posterior Interosseous Flap for Infected Posttraumatic Arthritis with an Active Fistula. A Rationale for Comprehensive Treatment. Case Report.\",\"authors\":\"Efraín Farías-Cisneros, Jorge Luis Martínez-Peniche, Luis Carlos Olguín-Delgado, Francisco Guillermo Castillo-Vázquez, Ranulfo Romo-Rodríguez, Armando Torres-Gómez\",\"doi\":\"10.1177/24715492221090745\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The indication for total elbow arthroplasty (TEA) for primary and posttraumatic elbow arthritis has increased, however, its indication after infection remains elusive. Wound closure about the elbow increases the challenge of treating a previously infected elbow, often necessitating soft tissue coverage with local or regional flaps. We present a 75-year-old male patient with an elbow infection following a failed complex intraarticular fracture open reduction and internal fixation of the distal humerus. Initially, he presented with severe functional impairment and pain, also with an active fistula with serous exudate, whose culture was positive for <i>Cutinebacterium acnes</i>. Septic hardware loosening, and septic nonunion with intraarticular involvement of the left elbow was diagnosed. The patient underwent hardware removal, fistulectomy, serial irrigation and debridement and a pedicled antegrade posterior interosseous artery (PIA) flap on staged surgical treatment. Finally, after ruling out infection persistence, a TEA was performed. We aim to report the outcome of a patient treated with a TEA in the context of a previously infected elbow with soft tissue coverage with an antegrade PIA flap. Comprehensive treatment must be done in an appropriate manner, to obtain an expedited and desirable outcome.</p>\",\"PeriodicalId\":73942,\"journal\":{\"name\":\"Journal of shoulder and elbow arthroplasty\",\"volume\":\"6 \",\"pages\":\"24715492221090745\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-03-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/a9/10.1177_24715492221090745.PMC9163731.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of shoulder and elbow arthroplasty\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/24715492221090745\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of shoulder and elbow arthroplasty","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24715492221090745","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Total Elbow Arthroplasty and Antegrade Posterior Interosseous Flap for Infected Posttraumatic Arthritis with an Active Fistula. A Rationale for Comprehensive Treatment. Case Report.
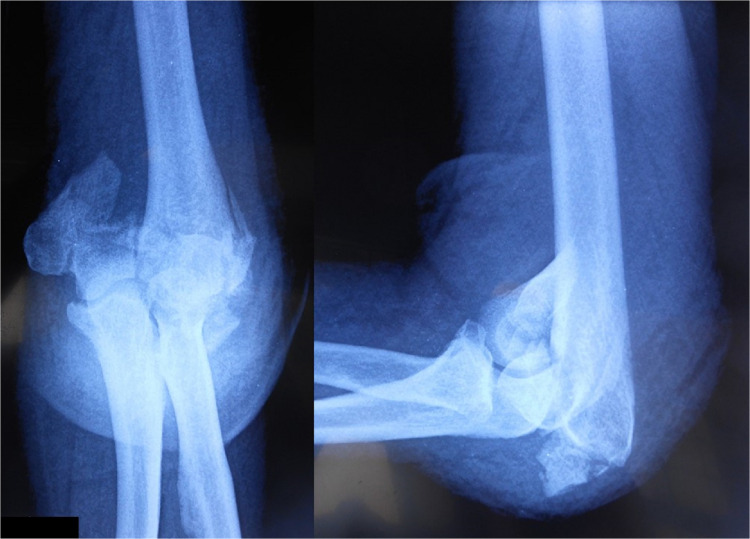
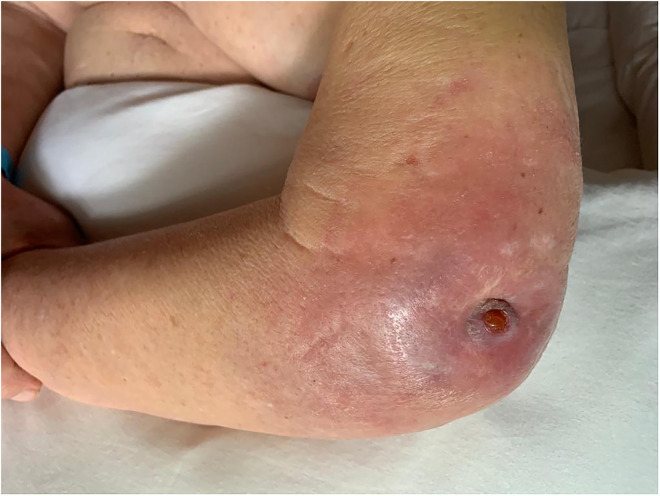
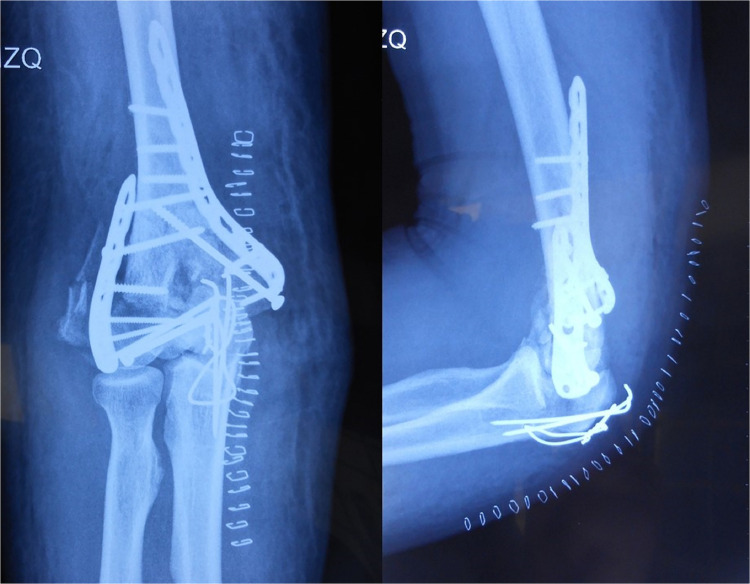
The indication for total elbow arthroplasty (TEA) for primary and posttraumatic elbow arthritis has increased, however, its indication after infection remains elusive. Wound closure about the elbow increases the challenge of treating a previously infected elbow, often necessitating soft tissue coverage with local or regional flaps. We present a 75-year-old male patient with an elbow infection following a failed complex intraarticular fracture open reduction and internal fixation of the distal humerus. Initially, he presented with severe functional impairment and pain, also with an active fistula with serous exudate, whose culture was positive for Cutinebacterium acnes. Septic hardware loosening, and septic nonunion with intraarticular involvement of the left elbow was diagnosed. The patient underwent hardware removal, fistulectomy, serial irrigation and debridement and a pedicled antegrade posterior interosseous artery (PIA) flap on staged surgical treatment. Finally, after ruling out infection persistence, a TEA was performed. We aim to report the outcome of a patient treated with a TEA in the context of a previously infected elbow with soft tissue coverage with an antegrade PIA flap. Comprehensive treatment must be done in an appropriate manner, to obtain an expedited and desirable outcome.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
