Marisa Gorrese, Roberto Guariglia, Annapaola Campana, Angela Bertolini, Lucia Fresolone, Maria Carmen Martorelli, Bianca Serio, Carmine Selleri, Valentina Giudice
{"title":"毛细胞白血病的双克隆性:具有不同表面膜免疫球蛋白表达的CD10+和CD10−克隆共现","authors":"Marisa Gorrese, Roberto Guariglia, Annapaola Campana, Angela Bertolini, Lucia Fresolone, Maria Carmen Martorelli, Bianca Serio, Carmine Selleri, Valentina Giudice","doi":"10.1002/cyto.b.22096","DOIUrl":null,"url":null,"abstract":"<p>Hairy cell leukemia (HCL), a rare indolent B-cell lymphoproliferative disorder, is characterized by the presence of bone marrow (BM) and peripheral blood hairy cells with cytoplasmic projections, splenomegaly, pancytopenia, and recurrent infections. In most cases, HCL cells harbor a V600E somatic mutation on B-raf proto-oncogene (<i>BRAF</i>), causing constitutive activation of downstream signaling pathways, especially mitogen-activated protein kinase (MEK) 1 and 2. Cytogenetics abnormalities can be also found, such as trisomy 5 and structural modifications on chromosomes 5 and 2, with no recurrent alteration, as well as Cyclin D1 overexpression (Maitre et al., <span>2022</span>). Classical HCL cells are characterized by surface expression of CD19, CD20, CD22, CD11c, CD25, CD79b, CD103, CD123, FMC7, and monoclonal light chain immunoglobulin (SmIg) restriction. These cells are typically negative for CD5, CD10, and CD23; however, CD10 positivity has been reported in 5%–14% of all HCL cases and CD23 positivity in 17%–21% of patients (Maitre et al., <span>2022</span>; Vittoria et al., <span>2021</span>). Therefore, HCL cell immunophenotype resembles that of post-germinal center B lymphocytes, also based on immunoglobulin (Ig) gene rearrangements. Biclonality in non-Hodgkin lymphomas is infrequent accounting for less than 5% of total cases, and in HCL is an even rarer event, only anecdotally reported (Vittoria et al., <span>2021</span>). We present a composite HCL case characterized by distinct expression of CD10 and SmIg. This case represented a diagnostic challenge, highlighting the need of multiparametric flow cytometry immunophenotyping for detection of subclones in lymphoproliferative disorders.</p><p>A 52 years-old male with obesity (BMI, 33) treated with gastric band in 2003 arrived at our observation in March 2022 for neutropenia (620 cells/μl) and thrombocytopenia (68,000 platelets/μl) with normal absolute lymphocyte count (2170 cells/μl) and hemoglobin levels (Hb, 13.4 g/dl; mean corpuscular volume [MCV], 100.8 fl). CT scan showed multiple lymphadenopathies located at the perivascular mediastinal region (aortic arch and left common carotid artery) with maximum diameter of 16 mm, and sub-centimetric left latero-cervical lymphadenopathies. Spleen enlargement (159 × 89 mm<sup>2</sup>) was also observed. BM biopsy showed a diffuse infiltration (60%) of medium-sized lymphoid cells with abundant cytoplasm and positive for CD20, PAX5, CD25, and CD10. Residual normal hemopoiesis was significantly reduced. Normal karyotype (46, XY) was documented by cytogenetic analysis performed on 20 mitoses, and the typical V600E <i>BRAF</i> mutation was observed by next-generation sequencing (variant allele frequency, 7.5%). Moreover, other several missense mutations of unknown significance were described on <i>TET2</i> (exon 3, Tyr867His and Pro3631Leu; and on exon 11, Leu1721Trp, Pro1723Ser, and His1778Arg), <i>SETBP1</i> (exon 4, Val231Leu, and Val1101Ile), and <i>JAK2</i> (exon 9, Leu393Val). BM aspirate displayed the presence of hairy cells, and residual hemopoiesis was mostly composed by erythroid precursors. Therefore, a diagnosis of HCL was made, and the patient was treated with pentostatin 4 mg/m<sup>2</sup> intravenously once every 2 weeks, as recommended.</p><p>For BM immunophenotyping, 50 μl of sample were stained with the following antibodies according to manufacturers' instructions: CD3 (APC), CD5 (PC7), CD19 (PC5.5), CD34 (APC700), CD16 (Pacific Blue), CD11b (PC7), CD13 (PC5.5), CD56 (ECD), CD45 (Krome Orange), CD33 (APC), HLA-DR (FITC), CD117 (PE), CD19 (ECD), SmIg-kappa (FITC), and SmIg-lambda (PE). HCL phenotype was characterized using the following antibodies: CD19 (ECD), CD20 (Pacific Blue), CD23 (PE), CD10 (PC7), CD22, FMC7 (FITC), CD103 (FITC), CD11c (PE), CD25 (PC5), CD49d (FITC), CD38 (PC7), CD43 (PE), and CD200 (PC7) (all from Beckman Coulter, Brea, CA). After incubation, red cell lysis was performed with IO Test Lysing Solution (Beckman Coulter), and cells were resuspended in 500 μl PBS for acquisition after two washings with PBS (IsoFlow Sheath Fluid, Beckman Coulter). Samples were acquired on a Navios EX cytometer (Beckman Coulter), equipped with violet (405 nm), blue (488 nm), and red (638 nm) lasers. Instrument daily quality control was performed using Flow-Check Pro Fluorospheres (Beckman Coulter), and external quality control by UK NEQAS for Leucocyte Immunophenotyping. Compensation was monthly checked as per clinical laboratory practice using flow-set and compensation kit (Beckman Coulter). Compensation was calculated using single-color controls for each fluorochrome and an unstained sample was used as negative control for setting PMT voltages. Samples were run using the same PMT voltages, and at least 1,000,000 events were recorded. Post-acquisition analysis was carried out using Kaluza C software (Beckman Coulter). For leukemic cell identification and myelogram, double cells were first removed using linear parameters and time; subsequently, cell populations were identified based on forward scatter area (FSC-A) and CD45 expression, and lymphocytes, monocytes, granulocytes, and immature cells were gated. Lymphocytes were further studied for T (CD3 or CD5 or CD7), B (CD19, SmIg-kappa, and SmIg-lambda), and natural killer (NK) cell (CD56 and CD16) markers. Normal CD34<sup>+</sup> cells were gated for CD19, CD117, and CD33 for definition of lymphoid (CD19<sup>+</sup>) or myeloid (CD117<sup>+</sup>CD33<sup>+</sup>) progenitors.</p><p>BM flow cytometry myelogram was composed by CD34<sup>+</sup> hematopoietic stem cells (0.1% of total nucleated cells), progenitors (3.7%), monocytes (0.2%), intermediate and mature granulocytes, T lymphocytes (30%), normal B cells (4%), and a HCL clone accounting for 39% of total leukocytes with the following immunophenotype: CD19<sup>++</sup>, CD45<sup>++</sup>, CD20<sup>+</sup> (99%), CD22<sup>+</sup> (98%), CD103<sup>+dim</sup> (98%), CD11c<sup>+bright</sup> (99%), CD25<sup>+</sup> (99%), CD10<sup>+/−</sup> (80%), CD5<sup>−</sup> (1%), CD23<sup>−</sup> (8%), FMC7<sup>+</sup> (99%), CD43<sup>−</sup> (3%), CD38<sup>−</sup> (1%), CD49d<sup>+</sup> (98%), CD200<sup>+bright</sup> (99%). Interestingly, when SmIg κ/λ analysis was performed on total CD19<sup>++</sup> pathologic cells, two different clones were identified. Indeed, cells with κ chain restriction (κ/λ, 98/2) were CD19<sup>++</sup>CD10<sup>+</sup>; conversely, cells with λ chain restriction (6/94) were CD19<sup>++</sup>CD10<sup>−</sup> and constituted a small pathological subclone (7% of total leukocytes) while the typical CD19<sup>++</sup>CD10<sup>+</sup> SmIg κ<sup>+</sup> population represented the dominant neoplastic clone (32% of total leukocytes) (Figure 1). In contrast with the other previously reported case of biclonal HCL, we were able to identify the two clones with opposite light chain restriction by flow cytometry based on the presence/absence of CD10 (Vittoria et al., <span>2021</span>).</p><p>At the time of writing, the patient was at the eighth cycle of therapy, and showed a partial remission with following blood counts: Hb levels, 9.9 g/dl; MCV, 99.4 fl; absolute neutrophil count, 690 cells/μl; platelet count, 114,000 platelets/μl; and absolute lymphocyte count, 320 cells/μl. By flow cytometry, minimal residual disease was 0.7% for the CD10<sup>+</sup>κ<sup>+</sup> clone, and 0.8% for the CD10<sup>−</sup>λ<sup>+</sup> clone.</p><p>CD10, a surface neutral endopeptidase, is a proliferation regulator of early BM B cell precursors and germinal center B lymphocytes, while it is not present on terminally differentiated plasma cells, and on pre- or post-germinal center B cells. CD10 is also expressed by various B cell diseases, such as precursor B cell acute lymphoblastic leukemia, follicular lymphoma, and germinal center-related diffuse large B-cell lymphomas. In humans, kappa chain rearrangement in pre-B cells occurs earlier than lambda chain, preceding IgM surface expression on immature B cells. In our case, the presence of two HCL clones that differ for CD10 expression and κ/λ restriction confirmed that neoplastic transformation occurs at the follicular/centroblast stage. Indeed, the predominant CD19<sup>++</sup>CD10<sup>+</sup> clone showed κ chain restriction, suggesting a more immature phenotype, while CD19<sup>++</sup>CD10<sup>−</sup> population displayed λ chain restriction, a more mature B cell phenotype. Moreover, two different lymphocyte populations were observed by peripheral blood smear morphology: one larger-sized hairy cells with eosinophilic granules, and another one of smaller-sized hairy cells with few cytoplasm.</p><p>In summary, once characterized the neoplastic clone, we suggest assessing κ/λ chain restriction by backgating on HCL cells to identify possible subclones with various surface antigen and light chain expression. The presence of two clones with opposite CD10 and κ/λ expression was a diagnostic challenge and raised a differential diagnosis of composite lymphomas co-occurrent with HCL. However, the two clones only varied for CD10 and κ/λ restriction, even though they showed different cell morphology. Awareness that HCL might be a composite lymphoproliferative disorder is needed for a better diagnosis and to understand clinical significance of this phenomenon.</p><p>Conceptualization: Valentina Giudice and Carmine Selleri; Clinical data: Roberto Guariglia, Maria Carmen Martorelli, and Bianca Serio; Flow cytometry analysis: Marisa Gorrese, Annapaola Campana, Angela Bertolini, and Lucia Fresolone; Writing-original draft preparation: Valentina Giudice and Marisa Gorrese; Writing-review and editing: Carmine Selleri. All authors have read and agreed to the published version of the manuscript.</p><p>The authors declare no conflicts of interest.</p><p>This article does not contain any studies with human participants or animals performed by any of the authors.</p><p>Patients received informed consent obtained in accordance with the Declaration of Helsinki (World Medical Association 2013) and protocols approved by local ethic committee (Ethics Committee “Campania Sud”, Brusciano, Naples, Italy; prot./SCCE n. 24988).</p>","PeriodicalId":10883,"journal":{"name":"Cytometry Part B: Clinical Cytometry","volume":"102 6","pages":"458-461"},"PeriodicalIF":2.7000,"publicationDate":"2022-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cyto.b.22096","citationCount":"2","resultStr":"{\"title\":\"Biclonality in hairy cell leukemia: Co-occurrence of CD10+ and CD10− clones with different surface membrane immunoglobulin expression\",\"authors\":\"Marisa Gorrese, Roberto Guariglia, Annapaola Campana, Angela Bertolini, Lucia Fresolone, Maria Carmen Martorelli, Bianca Serio, Carmine Selleri, Valentina Giudice\",\"doi\":\"10.1002/cyto.b.22096\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Hairy cell leukemia (HCL), a rare indolent B-cell lymphoproliferative disorder, is characterized by the presence of bone marrow (BM) and peripheral blood hairy cells with cytoplasmic projections, splenomegaly, pancytopenia, and recurrent infections. In most cases, HCL cells harbor a V600E somatic mutation on B-raf proto-oncogene (<i>BRAF</i>), causing constitutive activation of downstream signaling pathways, especially mitogen-activated protein kinase (MEK) 1 and 2. Cytogenetics abnormalities can be also found, such as trisomy 5 and structural modifications on chromosomes 5 and 2, with no recurrent alteration, as well as Cyclin D1 overexpression (Maitre et al., <span>2022</span>). Classical HCL cells are characterized by surface expression of CD19, CD20, CD22, CD11c, CD25, CD79b, CD103, CD123, FMC7, and monoclonal light chain immunoglobulin (SmIg) restriction. These cells are typically negative for CD5, CD10, and CD23; however, CD10 positivity has been reported in 5%–14% of all HCL cases and CD23 positivity in 17%–21% of patients (Maitre et al., <span>2022</span>; Vittoria et al., <span>2021</span>). Therefore, HCL cell immunophenotype resembles that of post-germinal center B lymphocytes, also based on immunoglobulin (Ig) gene rearrangements. Biclonality in non-Hodgkin lymphomas is infrequent accounting for less than 5% of total cases, and in HCL is an even rarer event, only anecdotally reported (Vittoria et al., <span>2021</span>). We present a composite HCL case characterized by distinct expression of CD10 and SmIg. This case represented a diagnostic challenge, highlighting the need of multiparametric flow cytometry immunophenotyping for detection of subclones in lymphoproliferative disorders.</p><p>A 52 years-old male with obesity (BMI, 33) treated with gastric band in 2003 arrived at our observation in March 2022 for neutropenia (620 cells/μl) and thrombocytopenia (68,000 platelets/μl) with normal absolute lymphocyte count (2170 cells/μl) and hemoglobin levels (Hb, 13.4 g/dl; mean corpuscular volume [MCV], 100.8 fl). CT scan showed multiple lymphadenopathies located at the perivascular mediastinal region (aortic arch and left common carotid artery) with maximum diameter of 16 mm, and sub-centimetric left latero-cervical lymphadenopathies. Spleen enlargement (159 × 89 mm<sup>2</sup>) was also observed. BM biopsy showed a diffuse infiltration (60%) of medium-sized lymphoid cells with abundant cytoplasm and positive for CD20, PAX5, CD25, and CD10. Residual normal hemopoiesis was significantly reduced. Normal karyotype (46, XY) was documented by cytogenetic analysis performed on 20 mitoses, and the typical V600E <i>BRAF</i> mutation was observed by next-generation sequencing (variant allele frequency, 7.5%). Moreover, other several missense mutations of unknown significance were described on <i>TET2</i> (exon 3, Tyr867His and Pro3631Leu; and on exon 11, Leu1721Trp, Pro1723Ser, and His1778Arg), <i>SETBP1</i> (exon 4, Val231Leu, and Val1101Ile), and <i>JAK2</i> (exon 9, Leu393Val). BM aspirate displayed the presence of hairy cells, and residual hemopoiesis was mostly composed by erythroid precursors. Therefore, a diagnosis of HCL was made, and the patient was treated with pentostatin 4 mg/m<sup>2</sup> intravenously once every 2 weeks, as recommended.</p><p>For BM immunophenotyping, 50 μl of sample were stained with the following antibodies according to manufacturers' instructions: CD3 (APC), CD5 (PC7), CD19 (PC5.5), CD34 (APC700), CD16 (Pacific Blue), CD11b (PC7), CD13 (PC5.5), CD56 (ECD), CD45 (Krome Orange), CD33 (APC), HLA-DR (FITC), CD117 (PE), CD19 (ECD), SmIg-kappa (FITC), and SmIg-lambda (PE). HCL phenotype was characterized using the following antibodies: CD19 (ECD), CD20 (Pacific Blue), CD23 (PE), CD10 (PC7), CD22, FMC7 (FITC), CD103 (FITC), CD11c (PE), CD25 (PC5), CD49d (FITC), CD38 (PC7), CD43 (PE), and CD200 (PC7) (all from Beckman Coulter, Brea, CA). After incubation, red cell lysis was performed with IO Test Lysing Solution (Beckman Coulter), and cells were resuspended in 500 μl PBS for acquisition after two washings with PBS (IsoFlow Sheath Fluid, Beckman Coulter). Samples were acquired on a Navios EX cytometer (Beckman Coulter), equipped with violet (405 nm), blue (488 nm), and red (638 nm) lasers. Instrument daily quality control was performed using Flow-Check Pro Fluorospheres (Beckman Coulter), and external quality control by UK NEQAS for Leucocyte Immunophenotyping. Compensation was monthly checked as per clinical laboratory practice using flow-set and compensation kit (Beckman Coulter). Compensation was calculated using single-color controls for each fluorochrome and an unstained sample was used as negative control for setting PMT voltages. Samples were run using the same PMT voltages, and at least 1,000,000 events were recorded. Post-acquisition analysis was carried out using Kaluza C software (Beckman Coulter). For leukemic cell identification and myelogram, double cells were first removed using linear parameters and time; subsequently, cell populations were identified based on forward scatter area (FSC-A) and CD45 expression, and lymphocytes, monocytes, granulocytes, and immature cells were gated. Lymphocytes were further studied for T (CD3 or CD5 or CD7), B (CD19, SmIg-kappa, and SmIg-lambda), and natural killer (NK) cell (CD56 and CD16) markers. Normal CD34<sup>+</sup> cells were gated for CD19, CD117, and CD33 for definition of lymphoid (CD19<sup>+</sup>) or myeloid (CD117<sup>+</sup>CD33<sup>+</sup>) progenitors.</p><p>BM flow cytometry myelogram was composed by CD34<sup>+</sup> hematopoietic stem cells (0.1% of total nucleated cells), progenitors (3.7%), monocytes (0.2%), intermediate and mature granulocytes, T lymphocytes (30%), normal B cells (4%), and a HCL clone accounting for 39% of total leukocytes with the following immunophenotype: CD19<sup>++</sup>, CD45<sup>++</sup>, CD20<sup>+</sup> (99%), CD22<sup>+</sup> (98%), CD103<sup>+dim</sup> (98%), CD11c<sup>+bright</sup> (99%), CD25<sup>+</sup> (99%), CD10<sup>+/−</sup> (80%), CD5<sup>−</sup> (1%), CD23<sup>−</sup> (8%), FMC7<sup>+</sup> (99%), CD43<sup>−</sup> (3%), CD38<sup>−</sup> (1%), CD49d<sup>+</sup> (98%), CD200<sup>+bright</sup> (99%). Interestingly, when SmIg κ/λ analysis was performed on total CD19<sup>++</sup> pathologic cells, two different clones were identified. Indeed, cells with κ chain restriction (κ/λ, 98/2) were CD19<sup>++</sup>CD10<sup>+</sup>; conversely, cells with λ chain restriction (6/94) were CD19<sup>++</sup>CD10<sup>−</sup> and constituted a small pathological subclone (7% of total leukocytes) while the typical CD19<sup>++</sup>CD10<sup>+</sup> SmIg κ<sup>+</sup> population represented the dominant neoplastic clone (32% of total leukocytes) (Figure 1). In contrast with the other previously reported case of biclonal HCL, we were able to identify the two clones with opposite light chain restriction by flow cytometry based on the presence/absence of CD10 (Vittoria et al., <span>2021</span>).</p><p>At the time of writing, the patient was at the eighth cycle of therapy, and showed a partial remission with following blood counts: Hb levels, 9.9 g/dl; MCV, 99.4 fl; absolute neutrophil count, 690 cells/μl; platelet count, 114,000 platelets/μl; and absolute lymphocyte count, 320 cells/μl. By flow cytometry, minimal residual disease was 0.7% for the CD10<sup>+</sup>κ<sup>+</sup> clone, and 0.8% for the CD10<sup>−</sup>λ<sup>+</sup> clone.</p><p>CD10, a surface neutral endopeptidase, is a proliferation regulator of early BM B cell precursors and germinal center B lymphocytes, while it is not present on terminally differentiated plasma cells, and on pre- or post-germinal center B cells. CD10 is also expressed by various B cell diseases, such as precursor B cell acute lymphoblastic leukemia, follicular lymphoma, and germinal center-related diffuse large B-cell lymphomas. In humans, kappa chain rearrangement in pre-B cells occurs earlier than lambda chain, preceding IgM surface expression on immature B cells. In our case, the presence of two HCL clones that differ for CD10 expression and κ/λ restriction confirmed that neoplastic transformation occurs at the follicular/centroblast stage. Indeed, the predominant CD19<sup>++</sup>CD10<sup>+</sup> clone showed κ chain restriction, suggesting a more immature phenotype, while CD19<sup>++</sup>CD10<sup>−</sup> population displayed λ chain restriction, a more mature B cell phenotype. Moreover, two different lymphocyte populations were observed by peripheral blood smear morphology: one larger-sized hairy cells with eosinophilic granules, and another one of smaller-sized hairy cells with few cytoplasm.</p><p>In summary, once characterized the neoplastic clone, we suggest assessing κ/λ chain restriction by backgating on HCL cells to identify possible subclones with various surface antigen and light chain expression. The presence of two clones with opposite CD10 and κ/λ expression was a diagnostic challenge and raised a differential diagnosis of composite lymphomas co-occurrent with HCL. However, the two clones only varied for CD10 and κ/λ restriction, even though they showed different cell morphology. Awareness that HCL might be a composite lymphoproliferative disorder is needed for a better diagnosis and to understand clinical significance of this phenomenon.</p><p>Conceptualization: Valentina Giudice and Carmine Selleri; Clinical data: Roberto Guariglia, Maria Carmen Martorelli, and Bianca Serio; Flow cytometry analysis: Marisa Gorrese, Annapaola Campana, Angela Bertolini, and Lucia Fresolone; Writing-original draft preparation: Valentina Giudice and Marisa Gorrese; Writing-review and editing: Carmine Selleri. All authors have read and agreed to the published version of the manuscript.</p><p>The authors declare no conflicts of interest.</p><p>This article does not contain any studies with human participants or animals performed by any of the authors.</p><p>Patients received informed consent obtained in accordance with the Declaration of Helsinki (World Medical Association 2013) and protocols approved by local ethic committee (Ethics Committee “Campania Sud”, Brusciano, Naples, Italy; prot./SCCE n. 24988).</p>\",\"PeriodicalId\":10883,\"journal\":{\"name\":\"Cytometry Part B: Clinical Cytometry\",\"volume\":\"102 6\",\"pages\":\"458-461\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2022-10-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cyto.b.22096\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cytometry Part B: Clinical Cytometry\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cyto.b.22096\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICAL LABORATORY TECHNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cytometry Part B: Clinical Cytometry","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cyto.b.22096","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICAL LABORATORY TECHNOLOGY","Score":null,"Total":0}
Biclonality in hairy cell leukemia: Co-occurrence of CD10+ and CD10− clones with different surface membrane immunoglobulin expression
Hairy cell leukemia (HCL), a rare indolent B-cell lymphoproliferative disorder, is characterized by the presence of bone marrow (BM) and peripheral blood hairy cells with cytoplasmic projections, splenomegaly, pancytopenia, and recurrent infections. In most cases, HCL cells harbor a V600E somatic mutation on B-raf proto-oncogene (BRAF), causing constitutive activation of downstream signaling pathways, especially mitogen-activated protein kinase (MEK) 1 and 2. Cytogenetics abnormalities can be also found, such as trisomy 5 and structural modifications on chromosomes 5 and 2, with no recurrent alteration, as well as Cyclin D1 overexpression (Maitre et al., 2022). Classical HCL cells are characterized by surface expression of CD19, CD20, CD22, CD11c, CD25, CD79b, CD103, CD123, FMC7, and monoclonal light chain immunoglobulin (SmIg) restriction. These cells are typically negative for CD5, CD10, and CD23; however, CD10 positivity has been reported in 5%–14% of all HCL cases and CD23 positivity in 17%–21% of patients (Maitre et al., 2022; Vittoria et al., 2021). Therefore, HCL cell immunophenotype resembles that of post-germinal center B lymphocytes, also based on immunoglobulin (Ig) gene rearrangements. Biclonality in non-Hodgkin lymphomas is infrequent accounting for less than 5% of total cases, and in HCL is an even rarer event, only anecdotally reported (Vittoria et al., 2021). We present a composite HCL case characterized by distinct expression of CD10 and SmIg. This case represented a diagnostic challenge, highlighting the need of multiparametric flow cytometry immunophenotyping for detection of subclones in lymphoproliferative disorders.
A 52 years-old male with obesity (BMI, 33) treated with gastric band in 2003 arrived at our observation in March 2022 for neutropenia (620 cells/μl) and thrombocytopenia (68,000 platelets/μl) with normal absolute lymphocyte count (2170 cells/μl) and hemoglobin levels (Hb, 13.4 g/dl; mean corpuscular volume [MCV], 100.8 fl). CT scan showed multiple lymphadenopathies located at the perivascular mediastinal region (aortic arch and left common carotid artery) with maximum diameter of 16 mm, and sub-centimetric left latero-cervical lymphadenopathies. Spleen enlargement (159 × 89 mm2) was also observed. BM biopsy showed a diffuse infiltration (60%) of medium-sized lymphoid cells with abundant cytoplasm and positive for CD20, PAX5, CD25, and CD10. Residual normal hemopoiesis was significantly reduced. Normal karyotype (46, XY) was documented by cytogenetic analysis performed on 20 mitoses, and the typical V600E BRAF mutation was observed by next-generation sequencing (variant allele frequency, 7.5%). Moreover, other several missense mutations of unknown significance were described on TET2 (exon 3, Tyr867His and Pro3631Leu; and on exon 11, Leu1721Trp, Pro1723Ser, and His1778Arg), SETBP1 (exon 4, Val231Leu, and Val1101Ile), and JAK2 (exon 9, Leu393Val). BM aspirate displayed the presence of hairy cells, and residual hemopoiesis was mostly composed by erythroid precursors. Therefore, a diagnosis of HCL was made, and the patient was treated with pentostatin 4 mg/m2 intravenously once every 2 weeks, as recommended.
For BM immunophenotyping, 50 μl of sample were stained with the following antibodies according to manufacturers' instructions: CD3 (APC), CD5 (PC7), CD19 (PC5.5), CD34 (APC700), CD16 (Pacific Blue), CD11b (PC7), CD13 (PC5.5), CD56 (ECD), CD45 (Krome Orange), CD33 (APC), HLA-DR (FITC), CD117 (PE), CD19 (ECD), SmIg-kappa (FITC), and SmIg-lambda (PE). HCL phenotype was characterized using the following antibodies: CD19 (ECD), CD20 (Pacific Blue), CD23 (PE), CD10 (PC7), CD22, FMC7 (FITC), CD103 (FITC), CD11c (PE), CD25 (PC5), CD49d (FITC), CD38 (PC7), CD43 (PE), and CD200 (PC7) (all from Beckman Coulter, Brea, CA). After incubation, red cell lysis was performed with IO Test Lysing Solution (Beckman Coulter), and cells were resuspended in 500 μl PBS for acquisition after two washings with PBS (IsoFlow Sheath Fluid, Beckman Coulter). Samples were acquired on a Navios EX cytometer (Beckman Coulter), equipped with violet (405 nm), blue (488 nm), and red (638 nm) lasers. Instrument daily quality control was performed using Flow-Check Pro Fluorospheres (Beckman Coulter), and external quality control by UK NEQAS for Leucocyte Immunophenotyping. Compensation was monthly checked as per clinical laboratory practice using flow-set and compensation kit (Beckman Coulter). Compensation was calculated using single-color controls for each fluorochrome and an unstained sample was used as negative control for setting PMT voltages. Samples were run using the same PMT voltages, and at least 1,000,000 events were recorded. Post-acquisition analysis was carried out using Kaluza C software (Beckman Coulter). For leukemic cell identification and myelogram, double cells were first removed using linear parameters and time; subsequently, cell populations were identified based on forward scatter area (FSC-A) and CD45 expression, and lymphocytes, monocytes, granulocytes, and immature cells were gated. Lymphocytes were further studied for T (CD3 or CD5 or CD7), B (CD19, SmIg-kappa, and SmIg-lambda), and natural killer (NK) cell (CD56 and CD16) markers. Normal CD34+ cells were gated for CD19, CD117, and CD33 for definition of lymphoid (CD19+) or myeloid (CD117+CD33+) progenitors.
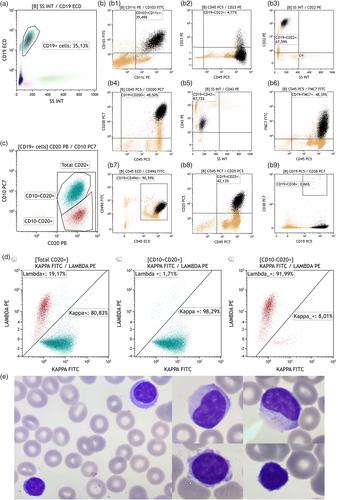
BM flow cytometry myelogram was composed by CD34+ hematopoietic stem cells (0.1% of total nucleated cells), progenitors (3.7%), monocytes (0.2%), intermediate and mature granulocytes, T lymphocytes (30%), normal B cells (4%), and a HCL clone accounting for 39% of total leukocytes with the following immunophenotype: CD19++, CD45++, CD20+ (99%), CD22+ (98%), CD103+dim (98%), CD11c+bright (99%), CD25+ (99%), CD10+/− (80%), CD5− (1%), CD23− (8%), FMC7+ (99%), CD43− (3%), CD38− (1%), CD49d+ (98%), CD200+bright (99%). Interestingly, when SmIg κ/λ analysis was performed on total CD19++ pathologic cells, two different clones were identified. Indeed, cells with κ chain restriction (κ/λ, 98/2) were CD19++CD10+; conversely, cells with λ chain restriction (6/94) were CD19++CD10− and constituted a small pathological subclone (7% of total leukocytes) while the typical CD19++CD10+ SmIg κ+ population represented the dominant neoplastic clone (32% of total leukocytes) (Figure 1). In contrast with the other previously reported case of biclonal HCL, we were able to identify the two clones with opposite light chain restriction by flow cytometry based on the presence/absence of CD10 (Vittoria et al., 2021).
At the time of writing, the patient was at the eighth cycle of therapy, and showed a partial remission with following blood counts: Hb levels, 9.9 g/dl; MCV, 99.4 fl; absolute neutrophil count, 690 cells/μl; platelet count, 114,000 platelets/μl; and absolute lymphocyte count, 320 cells/μl. By flow cytometry, minimal residual disease was 0.7% for the CD10+κ+ clone, and 0.8% for the CD10−λ+ clone.
CD10, a surface neutral endopeptidase, is a proliferation regulator of early BM B cell precursors and germinal center B lymphocytes, while it is not present on terminally differentiated plasma cells, and on pre- or post-germinal center B cells. CD10 is also expressed by various B cell diseases, such as precursor B cell acute lymphoblastic leukemia, follicular lymphoma, and germinal center-related diffuse large B-cell lymphomas. In humans, kappa chain rearrangement in pre-B cells occurs earlier than lambda chain, preceding IgM surface expression on immature B cells. In our case, the presence of two HCL clones that differ for CD10 expression and κ/λ restriction confirmed that neoplastic transformation occurs at the follicular/centroblast stage. Indeed, the predominant CD19++CD10+ clone showed κ chain restriction, suggesting a more immature phenotype, while CD19++CD10− population displayed λ chain restriction, a more mature B cell phenotype. Moreover, two different lymphocyte populations were observed by peripheral blood smear morphology: one larger-sized hairy cells with eosinophilic granules, and another one of smaller-sized hairy cells with few cytoplasm.
In summary, once characterized the neoplastic clone, we suggest assessing κ/λ chain restriction by backgating on HCL cells to identify possible subclones with various surface antigen and light chain expression. The presence of two clones with opposite CD10 and κ/λ expression was a diagnostic challenge and raised a differential diagnosis of composite lymphomas co-occurrent with HCL. However, the two clones only varied for CD10 and κ/λ restriction, even though they showed different cell morphology. Awareness that HCL might be a composite lymphoproliferative disorder is needed for a better diagnosis and to understand clinical significance of this phenomenon.
Conceptualization: Valentina Giudice and Carmine Selleri; Clinical data: Roberto Guariglia, Maria Carmen Martorelli, and Bianca Serio; Flow cytometry analysis: Marisa Gorrese, Annapaola Campana, Angela Bertolini, and Lucia Fresolone; Writing-original draft preparation: Valentina Giudice and Marisa Gorrese; Writing-review and editing: Carmine Selleri. All authors have read and agreed to the published version of the manuscript.
The authors declare no conflicts of interest.
This article does not contain any studies with human participants or animals performed by any of the authors.
Patients received informed consent obtained in accordance with the Declaration of Helsinki (World Medical Association 2013) and protocols approved by local ethic committee (Ethics Committee “Campania Sud”, Brusciano, Naples, Italy; prot./SCCE n. 24988).
期刊介绍:
Cytometry Part B: Clinical Cytometry features original research reports, in-depth reviews and special issues that directly relate to and palpably impact clinical flow, mass and image-based cytometry. These may include clinical and translational investigations important in the diagnostic, prognostic and therapeutic management of patients. Thus, we welcome research papers from various disciplines related [but not limited to] hematopathologists, hematologists, immunologists and cell biologists with clinically relevant and innovative studies investigating individual-cell analytics and/or separations. In addition to the types of papers indicated above, we also welcome Letters to the Editor, describing case reports or important medical or technical topics relevant to our readership without the length and depth of a full original report.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
