Raquel Ortigão, Brigitte Pereira, Rui Silva, Pedro Pimentel-Nunes, Pedro Bastos, Joaquim Abreu de Sousa, Filomena Faria, Mário Dinis-Ribeiro, Diogo Libânio
{"title":"食管癌和胃食管癌食管切除术后吻合口漏:多学科治疗是关键。","authors":"Raquel Ortigão, Brigitte Pereira, Rui Silva, Pedro Pimentel-Nunes, Pedro Bastos, Joaquim Abreu de Sousa, Filomena Faria, Mário Dinis-Ribeiro, Diogo Libânio","doi":"10.1159/000520562","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Anastomotic leakage after esophagectomy is associated with high mortality and impaired quality of life.</p><p><strong>Aim: </strong>The objective of this work was to determine the effectiveness of management of esophageal anastomotic leakage (EAL) after esophagectomy for esophageal and gastroesophageal junction (GEJ) cancer.</p><p><strong>Methods: </strong>Patients submitted to esophagectomy for esophageal and GEJ cancer at a tertiary oncology hospital between 2014 and 2019 (<i>n</i> = 119) were retrospectively reviewed and EAL risk factors and its management outcomes determined.</p><p><strong>Results: </strong>Older age and nodal disease were identified as independent risk factors for anastomotic leak (adjusted OR 1.06, 95% CI 1.00-1.13, and adjusted OR 4.89, 95% CI 1.09-21.8). Patients with EAL spent more days in the intensive care unit (ICU; median 14 vs. 4 days) and had higher 30-day mortality (15 vs. 2%) and higher in-hospital mortality (35 vs. 4%). The first treatment option was surgical in 13 patients, endoscopic in 10, and conservative in 3. No significant differences were noticeable between these patients, but sepsis and large leakages were tendentially managed by surgery. At follow-up, 3 patients in the surgery group (23%) and 9 in the endoscopic group (90%) were discharged under an oral diet (<i>p</i> = 0.001). The in-hospital mortality rate was 38% in the surgical group, 33% in the conservative group, and 10% in endoscopic group (<i>p</i> = 0.132). In patients with EAL, the presence of septic shock at leak diagnosis was the only predictor of mortality (<i>p</i> = 0.004). ICU length-of-stay was non-significantly lower in the endoscopic therapy group (median 4 days, vs. 16 days in the surgical group, <i>p</i> = 0.212).</p><p><strong>Conclusion: </strong>Risk factors for EAL may help change pre-procedural optimization. The results of this study suggest including an endoscopic approach for EAL.</p>","PeriodicalId":51838,"journal":{"name":"GE Portuguese Journal of Gastroenterology","volume":"30 1","pages":"38-48"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/c5/pjg-0030-0038.PMC9891149.pdf","citationCount":"1","resultStr":"{\"title\":\"Anastomotic Leaks following Esophagectomy for Esophageal and Gastroesophageal Junction Cancer: The Key Is the Multidisciplinary Management.\",\"authors\":\"Raquel Ortigão, Brigitte Pereira, Rui Silva, Pedro Pimentel-Nunes, Pedro Bastos, Joaquim Abreu de Sousa, Filomena Faria, Mário Dinis-Ribeiro, Diogo Libânio\",\"doi\":\"10.1159/000520562\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Anastomotic leakage after esophagectomy is associated with high mortality and impaired quality of life.</p><p><strong>Aim: </strong>The objective of this work was to determine the effectiveness of management of esophageal anastomotic leakage (EAL) after esophagectomy for esophageal and gastroesophageal junction (GEJ) cancer.</p><p><strong>Methods: </strong>Patients submitted to esophagectomy for esophageal and GEJ cancer at a tertiary oncology hospital between 2014 and 2019 (<i>n</i> = 119) were retrospectively reviewed and EAL risk factors and its management outcomes determined.</p><p><strong>Results: </strong>Older age and nodal disease were identified as independent risk factors for anastomotic leak (adjusted OR 1.06, 95% CI 1.00-1.13, and adjusted OR 4.89, 95% CI 1.09-21.8). Patients with EAL spent more days in the intensive care unit (ICU; median 14 vs. 4 days) and had higher 30-day mortality (15 vs. 2%) and higher in-hospital mortality (35 vs. 4%). The first treatment option was surgical in 13 patients, endoscopic in 10, and conservative in 3. No significant differences were noticeable between these patients, but sepsis and large leakages were tendentially managed by surgery. At follow-up, 3 patients in the surgery group (23%) and 9 in the endoscopic group (90%) were discharged under an oral diet (<i>p</i> = 0.001). The in-hospital mortality rate was 38% in the surgical group, 33% in the conservative group, and 10% in endoscopic group (<i>p</i> = 0.132). In patients with EAL, the presence of septic shock at leak diagnosis was the only predictor of mortality (<i>p</i> = 0.004). ICU length-of-stay was non-significantly lower in the endoscopic therapy group (median 4 days, vs. 16 days in the surgical group, <i>p</i> = 0.212).</p><p><strong>Conclusion: </strong>Risk factors for EAL may help change pre-procedural optimization. The results of this study suggest including an endoscopic approach for EAL.</p>\",\"PeriodicalId\":51838,\"journal\":{\"name\":\"GE Portuguese Journal of Gastroenterology\",\"volume\":\"30 1\",\"pages\":\"38-48\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/c5/pjg-0030-0038.PMC9891149.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GE Portuguese Journal of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000520562\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GE Portuguese Journal of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000520562","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
前言:食管切除术后吻合口瘘与高死亡率和生活质量下降有关。目的:本研究的目的是确定食管和胃食管交界处(GEJ)癌食管切除术后食管吻合口漏(EAL)的治疗效果。方法:回顾性分析2014年至2019年在某三级肿瘤医院因食管癌和GEJ癌行食管切除术的患者(n = 119),确定EAL的危险因素及其治疗结果。结果:年龄和淋巴结疾病被确定为吻合口漏的独立危险因素(校正OR 1.06, 95% CI 1.00-1.13,校正OR 4.89, 95% CI 1.09-21.8)。EAL患者在重症监护病房(ICU)的时间更长;中位14天对4天),30天死亡率较高(15天对2%),住院死亡率较高(35天对4%)。第一个治疗方案是手术治疗13例,内镜治疗10例,保守治疗3例。这些患者之间没有显著差异,但脓毒症和大泄漏倾向于手术治疗。随访时,手术组3例(23%)和内镜组9例(90%)患者在口服饮食下出院(p = 0.001)。手术组住院死亡率为38%,保守组为33%,内镜组为10% (p = 0.132)。在EAL患者中,脓毒性休克在泄漏诊断时是死亡率的唯一预测因子(p = 0.004)。内镜治疗组的ICU住院时间无显著性降低(中位4天,手术组为16天,p = 0.212)。结论:EAL的危险因素可能有助于术前优化。本研究的结果建议包括内窥镜入路EAL。
Anastomotic Leaks following Esophagectomy for Esophageal and Gastroesophageal Junction Cancer: The Key Is the Multidisciplinary Management.
Introduction: Anastomotic leakage after esophagectomy is associated with high mortality and impaired quality of life.
Aim: The objective of this work was to determine the effectiveness of management of esophageal anastomotic leakage (EAL) after esophagectomy for esophageal and gastroesophageal junction (GEJ) cancer.
Methods: Patients submitted to esophagectomy for esophageal and GEJ cancer at a tertiary oncology hospital between 2014 and 2019 (n = 119) were retrospectively reviewed and EAL risk factors and its management outcomes determined.
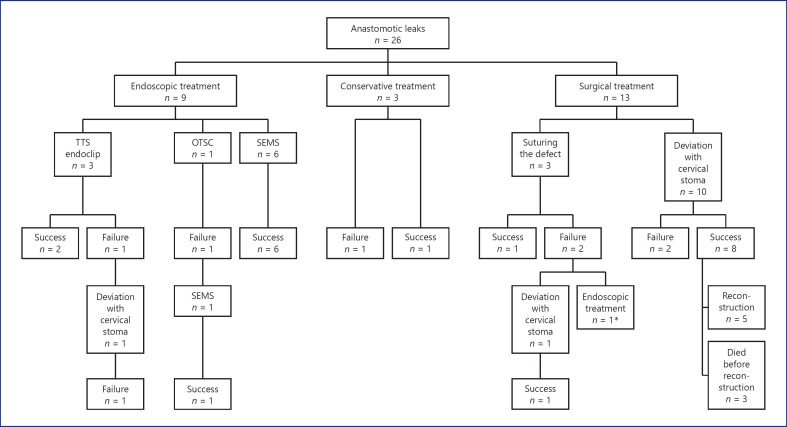
Results: Older age and nodal disease were identified as independent risk factors for anastomotic leak (adjusted OR 1.06, 95% CI 1.00-1.13, and adjusted OR 4.89, 95% CI 1.09-21.8). Patients with EAL spent more days in the intensive care unit (ICU; median 14 vs. 4 days) and had higher 30-day mortality (15 vs. 2%) and higher in-hospital mortality (35 vs. 4%). The first treatment option was surgical in 13 patients, endoscopic in 10, and conservative in 3. No significant differences were noticeable between these patients, but sepsis and large leakages were tendentially managed by surgery. At follow-up, 3 patients in the surgery group (23%) and 9 in the endoscopic group (90%) were discharged under an oral diet (p = 0.001). The in-hospital mortality rate was 38% in the surgical group, 33% in the conservative group, and 10% in endoscopic group (p = 0.132). In patients with EAL, the presence of septic shock at leak diagnosis was the only predictor of mortality (p = 0.004). ICU length-of-stay was non-significantly lower in the endoscopic therapy group (median 4 days, vs. 16 days in the surgical group, p = 0.212).
Conclusion: Risk factors for EAL may help change pre-procedural optimization. The results of this study suggest including an endoscopic approach for EAL.
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
