Ryan Malcolm Hum, Sarah Elyoussfi, Benjamin J Parker, Graeme Reid, Durga A K Kanigicherla
{"title":"igg4相关疾病和膜性肾病与含血栓反应蛋白1型结构域7A相关1例","authors":"Ryan Malcolm Hum, Sarah Elyoussfi, Benjamin J Parker, Graeme Reid, Durga A K Kanigicherla","doi":"10.1159/000524014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>IgG4-related disease (IgG4-RD) is a systemic multi-organ inflammatory disorder which affects the kidney 20% of the time. Patients with intrinsic IgG4-related kidney disease (IgG4-RKD) often have tubulointerstitial nephritis (TIN) whereas glomerular lesions like membranous nephropathy (MN) are less common. Antibodies to thrombospondin type-1 domain-containing 7A (THSD7A) have been described in primary MN, but never in association with IgG4-RKD.</p><p><strong>Case report: </strong>We report the first case of IgG4-MN associated with THSD7A antibodies in serum and positivity on glomerular staining, in a 57-year-old Caucasian male with IgG4-RD affecting the pancreas, liver, lacrimal glands, extraocular muscles, and kidneys. This patient presented initially with glomerular disease including significant proteinuria consistent with MN. Glomerular staining for THSD7A antigen and serum THSD7A antibody titres was positive. Treatment with corticosteroids and cyclophosphamide successfully induced remission with resolution of proteinuria, and improvement in renal function. However, despite maintenance azathioprine, the patient relapsed 39 months later. On relapse, there was minimal proteinuria but a significant rise in creatinine. Subsequent renal biopsy showed less glomerular disease and instead a TIN pattern. Subsequent treatment with Rituximab and corticosteroids successfully induced remission.</p><p><strong>Conclusion: </strong>The role of THSD7A autoantibodies in MN is emerging, and as both IgG4-MN and presence of THSD7A antibody are rare occurrences in themselves, we speculate that there may be an undiscovered association between THSD7A and IgG4-MN. Routine testing for THSD7A in IgG4-MN may help to identify the link.</p>","PeriodicalId":73177,"journal":{"name":"Glomerular diseases","volume":"2 3","pages":"139-144"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/3f/gdz-0002-0139.PMC9710322.pdf","citationCount":"1","resultStr":"{\"title\":\"A Case of IgG4-Related Disease and Membranous Nephropathy Associated with Thrombospondin Type-1 Domain-Containing 7A.\",\"authors\":\"Ryan Malcolm Hum, Sarah Elyoussfi, Benjamin J Parker, Graeme Reid, Durga A K Kanigicherla\",\"doi\":\"10.1159/000524014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>IgG4-related disease (IgG4-RD) is a systemic multi-organ inflammatory disorder which affects the kidney 20% of the time. Patients with intrinsic IgG4-related kidney disease (IgG4-RKD) often have tubulointerstitial nephritis (TIN) whereas glomerular lesions like membranous nephropathy (MN) are less common. Antibodies to thrombospondin type-1 domain-containing 7A (THSD7A) have been described in primary MN, but never in association with IgG4-RKD.</p><p><strong>Case report: </strong>We report the first case of IgG4-MN associated with THSD7A antibodies in serum and positivity on glomerular staining, in a 57-year-old Caucasian male with IgG4-RD affecting the pancreas, liver, lacrimal glands, extraocular muscles, and kidneys. This patient presented initially with glomerular disease including significant proteinuria consistent with MN. Glomerular staining for THSD7A antigen and serum THSD7A antibody titres was positive. Treatment with corticosteroids and cyclophosphamide successfully induced remission with resolution of proteinuria, and improvement in renal function. However, despite maintenance azathioprine, the patient relapsed 39 months later. On relapse, there was minimal proteinuria but a significant rise in creatinine. Subsequent renal biopsy showed less glomerular disease and instead a TIN pattern. Subsequent treatment with Rituximab and corticosteroids successfully induced remission.</p><p><strong>Conclusion: </strong>The role of THSD7A autoantibodies in MN is emerging, and as both IgG4-MN and presence of THSD7A antibody are rare occurrences in themselves, we speculate that there may be an undiscovered association between THSD7A and IgG4-MN. Routine testing for THSD7A in IgG4-MN may help to identify the link.</p>\",\"PeriodicalId\":73177,\"journal\":{\"name\":\"Glomerular diseases\",\"volume\":\"2 3\",\"pages\":\"139-144\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/3f/gdz-0002-0139.PMC9710322.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Glomerular diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000524014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Glomerular diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000524014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Case of IgG4-Related Disease and Membranous Nephropathy Associated with Thrombospondin Type-1 Domain-Containing 7A.
Background: IgG4-related disease (IgG4-RD) is a systemic multi-organ inflammatory disorder which affects the kidney 20% of the time. Patients with intrinsic IgG4-related kidney disease (IgG4-RKD) often have tubulointerstitial nephritis (TIN) whereas glomerular lesions like membranous nephropathy (MN) are less common. Antibodies to thrombospondin type-1 domain-containing 7A (THSD7A) have been described in primary MN, but never in association with IgG4-RKD.
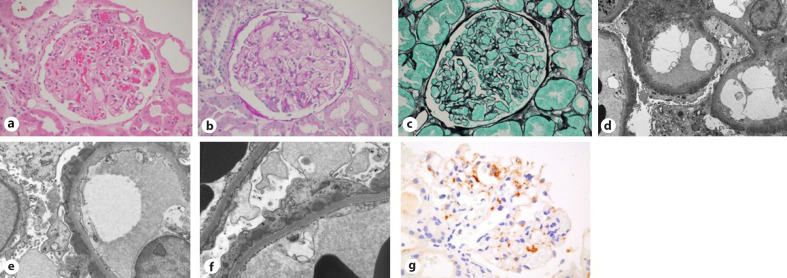
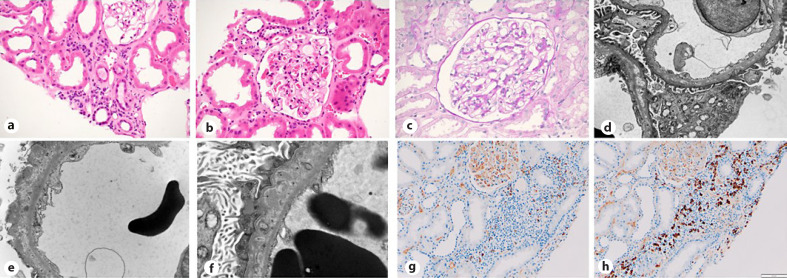
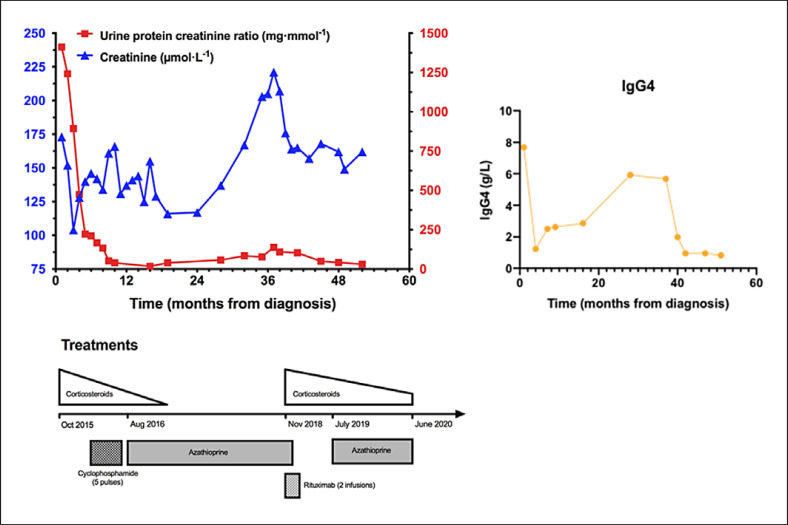
Case report: We report the first case of IgG4-MN associated with THSD7A antibodies in serum and positivity on glomerular staining, in a 57-year-old Caucasian male with IgG4-RD affecting the pancreas, liver, lacrimal glands, extraocular muscles, and kidneys. This patient presented initially with glomerular disease including significant proteinuria consistent with MN. Glomerular staining for THSD7A antigen and serum THSD7A antibody titres was positive. Treatment with corticosteroids and cyclophosphamide successfully induced remission with resolution of proteinuria, and improvement in renal function. However, despite maintenance azathioprine, the patient relapsed 39 months later. On relapse, there was minimal proteinuria but a significant rise in creatinine. Subsequent renal biopsy showed less glomerular disease and instead a TIN pattern. Subsequent treatment with Rituximab and corticosteroids successfully induced remission.
Conclusion: The role of THSD7A autoantibodies in MN is emerging, and as both IgG4-MN and presence of THSD7A antibody are rare occurrences in themselves, we speculate that there may be an undiscovered association between THSD7A and IgG4-MN. Routine testing for THSD7A in IgG4-MN may help to identify the link.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
