Gabriel B W Lerner, Gary G Singer, Christopher P Larsen, Tiffany N Caza
{"title":"免疫球蛋白阴性的原纤维性肾小球肾炎在糖尿病肾病中被掩盖:1例报告和诊断缺陷的讨论。","authors":"Gabriel B W Lerner, Gary G Singer, Christopher P Larsen, Tiffany N Caza","doi":"10.1159/000520071","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Fibrillary glomerulonephritis (FGN) is a rare glomerular disease with poor prognosis, characterized by deposition of randomly arranged fibrillar material measuring 10-30 nm in diameter. This diagnosis is confirmed with DNAJB9 immunohistochemistry as well as ultrastructural examination. Ultrastructurally, the fibrillary material seen in this entity may be confused with diabetic fibrillosis occurring in diabetic nephropathy.</p><p><strong>Case presentation: </strong>We present a case of a 63-year-old African American male with remote hepatitis C virus (HCV) infection and type II diabetes mellitus who presented with chronic kidney disease and nephrotic range proteinuria. A kidney biopsy revealed PAS-positive mesangial matrix expansion consistent with diabetic nephropathy and focal randomly oriented fibril deposition on ultrastructural examination. Immunofluorescence for immunoglobulin G and light chains was negative by both routine and paraffin immunofluorescence. Immunohistochemistry for DNAJB9 was diffusely positive, confirming co-existing FGN.</p><p><strong>Discussion/conclusion: </strong>Patients with diabetic nephropathy and FGN have similar clinicopathologic presentations with a slowly progressive onset of kidney failure and proteinuria. In diabetic patients with fibrillary deposits under ultrastructural examination, concurrence of these disease entities must be considered. In this patient with remote HCV infection that was successfully treated years before, it is possible that in the absence of an FGN trigger, there was a loss of antigenicity with a loss of immunoglobulin staining. Therefore, we recommend DNAJB9 immunostaining for patients with remote HCV infection to avoid this diagnostic pitfall. Further studies are needed to determine the potential role of HCV infection in the initiation and etiopathogenesis of FGN.</p>","PeriodicalId":73177,"journal":{"name":"Glomerular diseases","volume":"2 2","pages":"95-99"},"PeriodicalIF":0.0000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/c1/gdz-0002-0095.PMC9670039.pdf","citationCount":"1","resultStr":"{\"title\":\"Immunoglobulin-Negative Fibrillary Glomerulonephritis Masked in Diabetic Nephropathy: A Case Report and Discussion of a Diagnostic Pitfall.\",\"authors\":\"Gabriel B W Lerner, Gary G Singer, Christopher P Larsen, Tiffany N Caza\",\"doi\":\"10.1159/000520071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Fibrillary glomerulonephritis (FGN) is a rare glomerular disease with poor prognosis, characterized by deposition of randomly arranged fibrillar material measuring 10-30 nm in diameter. This diagnosis is confirmed with DNAJB9 immunohistochemistry as well as ultrastructural examination. Ultrastructurally, the fibrillary material seen in this entity may be confused with diabetic fibrillosis occurring in diabetic nephropathy.</p><p><strong>Case presentation: </strong>We present a case of a 63-year-old African American male with remote hepatitis C virus (HCV) infection and type II diabetes mellitus who presented with chronic kidney disease and nephrotic range proteinuria. A kidney biopsy revealed PAS-positive mesangial matrix expansion consistent with diabetic nephropathy and focal randomly oriented fibril deposition on ultrastructural examination. Immunofluorescence for immunoglobulin G and light chains was negative by both routine and paraffin immunofluorescence. Immunohistochemistry for DNAJB9 was diffusely positive, confirming co-existing FGN.</p><p><strong>Discussion/conclusion: </strong>Patients with diabetic nephropathy and FGN have similar clinicopathologic presentations with a slowly progressive onset of kidney failure and proteinuria. In diabetic patients with fibrillary deposits under ultrastructural examination, concurrence of these disease entities must be considered. In this patient with remote HCV infection that was successfully treated years before, it is possible that in the absence of an FGN trigger, there was a loss of antigenicity with a loss of immunoglobulin staining. Therefore, we recommend DNAJB9 immunostaining for patients with remote HCV infection to avoid this diagnostic pitfall. Further studies are needed to determine the potential role of HCV infection in the initiation and etiopathogenesis of FGN.</p>\",\"PeriodicalId\":73177,\"journal\":{\"name\":\"Glomerular diseases\",\"volume\":\"2 2\",\"pages\":\"95-99\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/c1/gdz-0002-0095.PMC9670039.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Glomerular diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000520071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Glomerular diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000520071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Immunoglobulin-Negative Fibrillary Glomerulonephritis Masked in Diabetic Nephropathy: A Case Report and Discussion of a Diagnostic Pitfall.
Introduction: Fibrillary glomerulonephritis (FGN) is a rare glomerular disease with poor prognosis, characterized by deposition of randomly arranged fibrillar material measuring 10-30 nm in diameter. This diagnosis is confirmed with DNAJB9 immunohistochemistry as well as ultrastructural examination. Ultrastructurally, the fibrillary material seen in this entity may be confused with diabetic fibrillosis occurring in diabetic nephropathy.
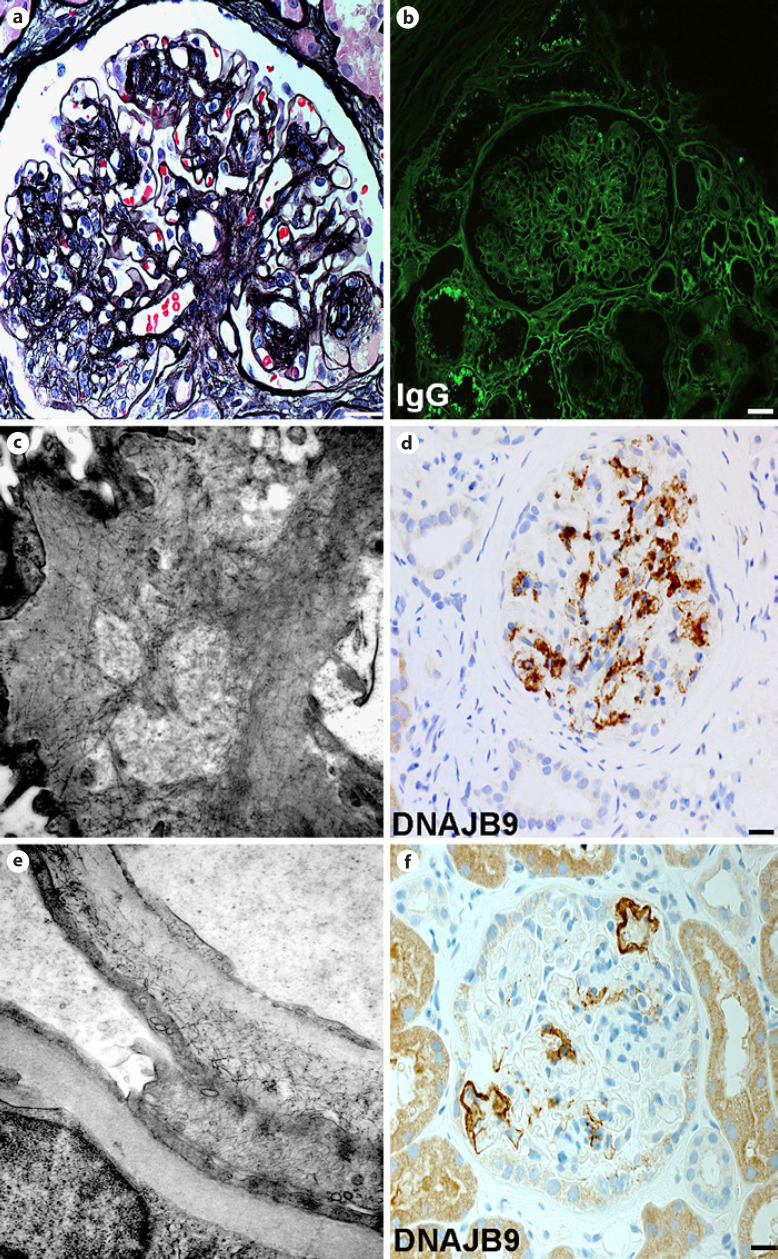
Case presentation: We present a case of a 63-year-old African American male with remote hepatitis C virus (HCV) infection and type II diabetes mellitus who presented with chronic kidney disease and nephrotic range proteinuria. A kidney biopsy revealed PAS-positive mesangial matrix expansion consistent with diabetic nephropathy and focal randomly oriented fibril deposition on ultrastructural examination. Immunofluorescence for immunoglobulin G and light chains was negative by both routine and paraffin immunofluorescence. Immunohistochemistry for DNAJB9 was diffusely positive, confirming co-existing FGN.
Discussion/conclusion: Patients with diabetic nephropathy and FGN have similar clinicopathologic presentations with a slowly progressive onset of kidney failure and proteinuria. In diabetic patients with fibrillary deposits under ultrastructural examination, concurrence of these disease entities must be considered. In this patient with remote HCV infection that was successfully treated years before, it is possible that in the absence of an FGN trigger, there was a loss of antigenicity with a loss of immunoglobulin staining. Therefore, we recommend DNAJB9 immunostaining for patients with remote HCV infection to avoid this diagnostic pitfall. Further studies are needed to determine the potential role of HCV infection in the initiation and etiopathogenesis of FGN.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
