Alexandros Rodolakis, Giovanni Scambia, François Planchamp, Maribel Acien, Attilio Di Spiezio Sardo, Martin Farrugia, Michael Grynberg, Maja Pakiz, Kitty Pavlakis, Nathalie Vermeulen, Gianfranco Zannoni, Ignacio Zapardiel, Kirsten Louise Tryde Macklon
{"title":"子宫内膜癌患者保留生育能力治疗的ESGO/ESHRE/ESGE指南","authors":"Alexandros Rodolakis, Giovanni Scambia, François Planchamp, Maribel Acien, Attilio Di Spiezio Sardo, Martin Farrugia, Michael Grynberg, Maja Pakiz, Kitty Pavlakis, Nathalie Vermeulen, Gianfranco Zannoni, Ignacio Zapardiel, Kirsten Louise Tryde Macklon","doi":"10.1093/hropen/hoac057","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>How should fertility-sparing treatment of patients with endometrial carcinoma be performed?</p><p><strong>Summary answer: </strong>Forty-eight recommendations were formulated on fertility-sparing treatment of patients with endometrial carcinoma.</p><p><strong>What is known already: </strong>The standard surgical treatment of endometrial carcinoma consisting of total hysterectomy with bilateral salpingo-oophorectomy drastically affects the quality of life of patients and creates a challenge for clinicians. Recent evidence-based guidelines of the European Society of Gynaecological Oncology (ESGO), the European SocieTy for Radiotherapy & Oncology (ESTRO) and the European Society of Pathology (ESP) provide comprehensive guidelines on all relevant issues of diagnosis and treatment in endometrial carcinoma in a multidisciplinary setting. While addressing also work-up for fertility preservation treatments and the management and follow-up for fertility preservation, it was considered relevant to further extend the guidance on fertility-sparing treatment.</p><p><strong>Study design size duration: </strong>A collaboration was set up between the ESGO, the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), aiming to develop clinically relevant and evidence-based guidelines focusing on key aspects of fertility-sparing treatment in order to improve the quality of care for women with endometrial carcinoma across Europe and worldwide.</p><p><strong>Participants/materials setting methods: </strong>ESGO/ESHRE/ESGE nominated an international multidisciplinary development group consisting of practising clinicians and researchers who have demonstrated leadership and expertise in the care and research of endometrial carcinoma (11 experts across Europe). To ensure that the guidelines are evidence-based, the literature published since 2016, identified from a systematic search was reviewed and critically appraised. In the absence of any clear scientific evidence, judgement was based on the professional experience and consensus of the development group. The guidelines are thus based on the best available evidence and expert agreement. Prior to publication, the guidelines were reviewed by 95 independent international practitioners in cancer care delivery and patient representatives.</p><p><strong>Main results and the role of chance: </strong>The multidisciplinary development group formulated 48 recommendations in four sections; patient selection, tumour clinicopathological characteristics, treatment and special issues.</p><p><strong>Limitations reasons for caution: </strong>Of the 48 recommendations, none could be based on level I evidence and only 16 could be based on level II evidence, implicating that 66% of the recommendations are supported only by observational data, professional experience and consensus of the development group.</p><p><strong>Wider implications of the findings: </strong>These recommendations provide guidance to professionals caring for women with endometrial carcinoma, including but not limited to professionals in the field of gynaecological oncology, onco-fertility, reproductive surgery, endoscopy, conservative surgery and histopathology, and will help towards a holistic and multidisciplinary approach for this challenging clinical scenario.</p><p><strong>Study funding/competing interests: </strong>All costs relating to the development process were covered from ESGO, ESHRE and ESGE funds. There was no external funding of the development process or manuscript production. G.S. has reported grants from MSD Italia S.r.l., advisory boards for Storz, Bayer, Astrazeneca, Metronic, TESARO Bio Italy S.r.l and Johnson & Johnson, and honoraria for lectures from Clovis Oncology Italy S.r.l. M.G. has reported advisory boards for Gedeon Richter and Merck. The other authors have reported no conflicts of interest.</p><p><strong>Disclaimer: </strong><i>This document represents the views of ESHRE, ESGO and ESGE which are the result of consensus between the relevant stakeholders and where relevant based on the scientific evidence available at the time of preparation</i>. <i>The recommendations should be used for informational and educational purposes. They should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care nor exclusive of other methods of care reasonably directed to obtaining the same results. They do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type</i>.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 1","pages":"hoac057"},"PeriodicalIF":8.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9900425/pdf/","citationCount":"4","resultStr":"{\"title\":\"ESGO/ESHRE/ESGE Guidelines for the fertility-sparing treatment of patients with endometrial carcinoma<sup />.\",\"authors\":\"Alexandros Rodolakis, Giovanni Scambia, François Planchamp, Maribel Acien, Attilio Di Spiezio Sardo, Martin Farrugia, Michael Grynberg, Maja Pakiz, Kitty Pavlakis, Nathalie Vermeulen, Gianfranco Zannoni, Ignacio Zapardiel, Kirsten Louise Tryde Macklon\",\"doi\":\"10.1093/hropen/hoac057\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>How should fertility-sparing treatment of patients with endometrial carcinoma be performed?</p><p><strong>Summary answer: </strong>Forty-eight recommendations were formulated on fertility-sparing treatment of patients with endometrial carcinoma.</p><p><strong>What is known already: </strong>The standard surgical treatment of endometrial carcinoma consisting of total hysterectomy with bilateral salpingo-oophorectomy drastically affects the quality of life of patients and creates a challenge for clinicians. Recent evidence-based guidelines of the European Society of Gynaecological Oncology (ESGO), the European SocieTy for Radiotherapy & Oncology (ESTRO) and the European Society of Pathology (ESP) provide comprehensive guidelines on all relevant issues of diagnosis and treatment in endometrial carcinoma in a multidisciplinary setting. While addressing also work-up for fertility preservation treatments and the management and follow-up for fertility preservation, it was considered relevant to further extend the guidance on fertility-sparing treatment.</p><p><strong>Study design size duration: </strong>A collaboration was set up between the ESGO, the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), aiming to develop clinically relevant and evidence-based guidelines focusing on key aspects of fertility-sparing treatment in order to improve the quality of care for women with endometrial carcinoma across Europe and worldwide.</p><p><strong>Participants/materials setting methods: </strong>ESGO/ESHRE/ESGE nominated an international multidisciplinary development group consisting of practising clinicians and researchers who have demonstrated leadership and expertise in the care and research of endometrial carcinoma (11 experts across Europe). To ensure that the guidelines are evidence-based, the literature published since 2016, identified from a systematic search was reviewed and critically appraised. In the absence of any clear scientific evidence, judgement was based on the professional experience and consensus of the development group. The guidelines are thus based on the best available evidence and expert agreement. Prior to publication, the guidelines were reviewed by 95 independent international practitioners in cancer care delivery and patient representatives.</p><p><strong>Main results and the role of chance: </strong>The multidisciplinary development group formulated 48 recommendations in four sections; patient selection, tumour clinicopathological characteristics, treatment and special issues.</p><p><strong>Limitations reasons for caution: </strong>Of the 48 recommendations, none could be based on level I evidence and only 16 could be based on level II evidence, implicating that 66% of the recommendations are supported only by observational data, professional experience and consensus of the development group.</p><p><strong>Wider implications of the findings: </strong>These recommendations provide guidance to professionals caring for women with endometrial carcinoma, including but not limited to professionals in the field of gynaecological oncology, onco-fertility, reproductive surgery, endoscopy, conservative surgery and histopathology, and will help towards a holistic and multidisciplinary approach for this challenging clinical scenario.</p><p><strong>Study funding/competing interests: </strong>All costs relating to the development process were covered from ESGO, ESHRE and ESGE funds. There was no external funding of the development process or manuscript production. G.S. has reported grants from MSD Italia S.r.l., advisory boards for Storz, Bayer, Astrazeneca, Metronic, TESARO Bio Italy S.r.l and Johnson & Johnson, and honoraria for lectures from Clovis Oncology Italy S.r.l. M.G. has reported advisory boards for Gedeon Richter and Merck. The other authors have reported no conflicts of interest.</p><p><strong>Disclaimer: </strong><i>This document represents the views of ESHRE, ESGO and ESGE which are the result of consensus between the relevant stakeholders and where relevant based on the scientific evidence available at the time of preparation</i>. <i>The recommendations should be used for informational and educational purposes. They should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care nor exclusive of other methods of care reasonably directed to obtaining the same results. They do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type</i>.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2023 1\",\"pages\":\"hoac057\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9900425/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoac057\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoac057","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 4
摘要
研究问题:子宫内膜癌患者应如何进行保留生育能力的治疗?总结回答:对子宫内膜癌患者保留生育能力的治疗提出了48条建议。已知情况:子宫内膜癌的标准手术治疗包括全子宫切除术和双侧输卵管-卵巢切除术,这极大地影响了患者的生活质量,给临床医生带来了挑战。最近,欧洲妇科肿瘤学会(ESGO)、欧洲放射与肿瘤学会(ESTRO)和欧洲病理学会(ESP)的循证指南为多学科背景下子宫内膜癌诊断和治疗的所有相关问题提供了全面的指南。在处理保留生育能力治疗的后继工作和保留生育能力的管理和后续工作的同时,认为有必要进一步扩大保留生育能力治疗的指导。研究设计规模持续时间:ESGO、欧洲人类生殖与胚胎学会(ESHRE)和欧洲妇科内窥镜学会(ESGE)之间建立了一项合作,旨在制定临床相关的循证指南,重点关注生育保留治疗的关键方面,以提高欧洲和全球子宫内膜癌女性的护理质量。参与者/材料设置方法:ESGO/ESHRE/ESGE提名了一个国际多学科发展小组,由在子宫内膜癌的护理和研究方面表现出领导力和专业知识的执业临床医生和研究人员组成(来自欧洲的11名专家)。为了确保指南以证据为基础,对2016年以来发表的文献进行了审查和批判性评估,这些文献是通过系统检索确定的。在没有任何明确的科学证据的情况下,判断是基于专业经验和发展小组的共识。因此,该指南是基于现有的最佳证据和专家协议。在发表之前,该指南由95名独立的国际癌症护理从业人员和患者代表进行了审查。主要结果和机遇的作用:多学科发展小组在四个部分提出了48条建议;患者选择,肿瘤临床病理特征,治疗和特殊问题。谨慎的局限性:在48条建议中,没有一条可基于一级证据,只有16条可基于二级证据,这意味着66%的建议仅由观察数据、专业经验和发展小组的共识支持。研究结果的更广泛意义:这些建议为照顾子宫内膜癌妇女的专业人员提供指导,包括但不限于妇科肿瘤学、肿瘤生育、生殖外科、内窥镜检查、保守手术和组织病理学领域的专业人员,并将有助于为这一具有挑战性的临床情况提供全面和多学科的方法。研究经费/竞争利益:与开发过程有关的所有费用均由ESGO、ESHRE和ESGE基金支付。没有外部资金支持开发过程或手稿制作。G.S.获得了MSD Italia S.r.l、Storz、Bayer、Astrazeneca、Metronic、TESARO Bio Italy S.r.l和Johnson & Johnson顾问委员会的资助,并获得了Clovis Oncology Italy S.r.l的讲座荣誉。M.G.还获得了Gedeon Richter和Merck顾问委员会的报告。其他作者没有报告任何利益冲突。免责声明:本文件代表ESHRE、ESGO和ESGE的观点,是相关利益相关者之间达成共识的结果,并在相关情况下基于准备时可用的科学证据。这些建议应用于宣传和教育目的。它们不应被解释为制定护理标准,也不应被视为包括所有适当的护理方法,也不应排除其他合理指导以获得相同结果的护理方法。它们不能取代对每个个体表现的临床判断,也不能取代基于地点和设施类型的变化。
ESGO/ESHRE/ESGE Guidelines for the fertility-sparing treatment of patients with endometrial carcinoma.
Study question: How should fertility-sparing treatment of patients with endometrial carcinoma be performed?
Summary answer: Forty-eight recommendations were formulated on fertility-sparing treatment of patients with endometrial carcinoma.
What is known already: The standard surgical treatment of endometrial carcinoma consisting of total hysterectomy with bilateral salpingo-oophorectomy drastically affects the quality of life of patients and creates a challenge for clinicians. Recent evidence-based guidelines of the European Society of Gynaecological Oncology (ESGO), the European SocieTy for Radiotherapy & Oncology (ESTRO) and the European Society of Pathology (ESP) provide comprehensive guidelines on all relevant issues of diagnosis and treatment in endometrial carcinoma in a multidisciplinary setting. While addressing also work-up for fertility preservation treatments and the management and follow-up for fertility preservation, it was considered relevant to further extend the guidance on fertility-sparing treatment.
Study design size duration: A collaboration was set up between the ESGO, the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), aiming to develop clinically relevant and evidence-based guidelines focusing on key aspects of fertility-sparing treatment in order to improve the quality of care for women with endometrial carcinoma across Europe and worldwide.
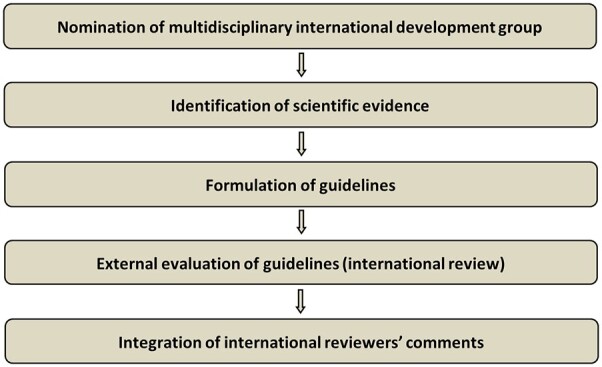
Participants/materials setting methods: ESGO/ESHRE/ESGE nominated an international multidisciplinary development group consisting of practising clinicians and researchers who have demonstrated leadership and expertise in the care and research of endometrial carcinoma (11 experts across Europe). To ensure that the guidelines are evidence-based, the literature published since 2016, identified from a systematic search was reviewed and critically appraised. In the absence of any clear scientific evidence, judgement was based on the professional experience and consensus of the development group. The guidelines are thus based on the best available evidence and expert agreement. Prior to publication, the guidelines were reviewed by 95 independent international practitioners in cancer care delivery and patient representatives.
Main results and the role of chance: The multidisciplinary development group formulated 48 recommendations in four sections; patient selection, tumour clinicopathological characteristics, treatment and special issues.
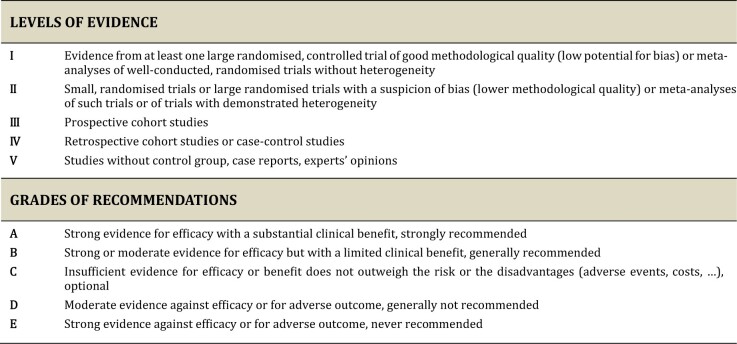
Limitations reasons for caution: Of the 48 recommendations, none could be based on level I evidence and only 16 could be based on level II evidence, implicating that 66% of the recommendations are supported only by observational data, professional experience and consensus of the development group.
Wider implications of the findings: These recommendations provide guidance to professionals caring for women with endometrial carcinoma, including but not limited to professionals in the field of gynaecological oncology, onco-fertility, reproductive surgery, endoscopy, conservative surgery and histopathology, and will help towards a holistic and multidisciplinary approach for this challenging clinical scenario.
Study funding/competing interests: All costs relating to the development process were covered from ESGO, ESHRE and ESGE funds. There was no external funding of the development process or manuscript production. G.S. has reported grants from MSD Italia S.r.l., advisory boards for Storz, Bayer, Astrazeneca, Metronic, TESARO Bio Italy S.r.l and Johnson & Johnson, and honoraria for lectures from Clovis Oncology Italy S.r.l. M.G. has reported advisory boards for Gedeon Richter and Merck. The other authors have reported no conflicts of interest.
Disclaimer: This document represents the views of ESHRE, ESGO and ESGE which are the result of consensus between the relevant stakeholders and where relevant based on the scientific evidence available at the time of preparation. The recommendations should be used for informational and educational purposes. They should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care nor exclusive of other methods of care reasonably directed to obtaining the same results. They do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
