Xiaoyan Li, Xin Yuan, Zhe Xu, Lei Shi, Lei Huang, Xuechun Lu, Junliang Fu
{"title":"甲基强的松龙对重症 COVID-19 患者死亡率和临床病程的影响:倾向得分匹配分析","authors":"Xiaoyan Li, Xin Yuan, Zhe Xu, Lei Shi, Lei Huang, Xuechun Lu, Junliang Fu","doi":"10.1097/ID9.0000000000000076","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Whether methylprednisolone therapy can reduce the mortality rate of patients with severe coronavirus disease 2019 (COVID-19) remains controversial, and its effects on the length of hospital stay and virus shedding time are also unknown. This retrospective study investigates the previous issues to provide more evidence for methylprednisolone treatment in severe COVID-19.</p><p><strong>Methods: </strong>This retrospective study included 563 of 4827 patients with confirmed COVID-19 admitted to Wuhan Huoshenshan Hospital or Wuhan Guanggu Hospital between February 3, 2020 and March 30, 2020 who met the screening criteria. The participants' epidemiological and demographic data, comorbidities, laboratory test results, treatments, outcomes, and vital clinical time points were extracted from electronic medical records. The primary outcome was in-hospital death, and the secondary outcomes were 2 clinical courses: length from admission to viral clearance and discharge. Univariate and multivariate logistic or linear regression analyses were used to assess the role of methylprednisolone in different outcomes. Propensity score matching was performed to control for confounding factors.</p><p><strong>Results: </strong>Of the 563 patients who met the screening criteria and were included in the subsequent analysis, 138 were included in the methylprednisolone group and 425 in the nonmethylprednisolone group. The in-hospital death rate between the methylprednisolone and nonmethylprednisolone groups showed a significant difference (23.91% <i>vs.</i> 1.65%, <i>P</i> < 0.001), which was maintained after propensity score matching (13.98% <i>vs.</i> 5.38%, <i>P</i> = 0.048). However, univariate logistic analysis in the matched groups showed that methylprednisolone treatment (odds ratio [OR], 5.242; 95% confidence interval [CI], 0.802 to 34.246; <i>P</i> = 0.084) was not a risk factor for in-hospital death in severe patients. Further multivariate logistic regression analysis found comorbidities (OR, 3.327; 95% CI, 1.702 to 6.501; <i>P</i> < 0.001), lower lymphocyte count (OR, 0.076; 95% CI, 0.012 to 0.461; <i>P</i> = 0.005), higher lactate dehydrogenase (LDH) levels (OR, 1.008; 95% CI, 1.003 to 1.013; <i>P</i> = 0.002), and anticoagulation therapy (OR, 11.187; 95% CI, 2.459 to 50.900; <i>P</i> = 0.002) were associated with in-hospital mortality. Multivariate linear regression analysis in the matched groups showed that methylprednisolone treatment was not a risk factor for a prolonged duration from admission to viral clearance (β Value 0.081; 95% CI, -1.012 to 3.657; <i>P</i> = 0.265) or discharge (β Value 0.114; 95% CI, -0.723 to 6.408; <i>P</i> = 0.117). d-dimer (β Value, 0.144; 95% CI, 0.012 to 0.817; <i>P</i> = 0.044), LDH (β Value 0.260; 95% CI, 0.010 to 0.034; <i>P</i> < 0.001), and antiviral therapy (β Value 0.220; 95% CI, 1.373 to 6.263; <i>P</i> = 0.002) were associated with a longer length from admission to viral clearance. The lymphocyte count (β Value -0.206; 95% CI, -6.248 to -1.197; <i>P</i> = 0.004), LDH (β Value 0.231; 95% CI, 0.012 to 0.048; <i>P</i> = 0.001), antiviral therapy (β Value 0.143; 95% CI, 0.058 to 7.497; <i>P</i> = 0.047), and antibacterial therapy (β Value 0.152; 95% CI, 0.133 to 8.154; <i>P</i> = 0.043) were associated with a longer hospitalization duration from admission to discharge. Further stratified analysis revealed that the low daily dose group (≤60 mg/d) and the low total dose group (≤200 mg) had shorter duration from admission to viral clearance (Z=-2.362, <i>P</i> = 0.018; Z=-2.010, <i>P</i> = 0.044) and a shorter hospital stay (Z=-2.735, <i>P</i> = 0.006; Z=-3.858, <i>P</i> < 0.001).</p><p><strong>Conclusions: </strong>In patients with severe COVID-19, methylprednisolone is safe and does not prolong the duration from admission to viral clearance or discharge. Low-dose, short-term methylprednisolone treatment may be more beneficial in shortening the disease course.</p>","PeriodicalId":73371,"journal":{"name":"Infectious diseases & immunity","volume":"3 1","pages":"20-28"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/72/84/idi-3-20.PMC9912987.pdf","citationCount":"0","resultStr":"{\"title\":\"Effect of Methylprednisolone on Mortality and Clinical Courses in Patients with Severe COVID-19: A Propensity Score Matching Analysis.\",\"authors\":\"Xiaoyan Li, Xin Yuan, Zhe Xu, Lei Shi, Lei Huang, Xuechun Lu, Junliang Fu\",\"doi\":\"10.1097/ID9.0000000000000076\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Whether methylprednisolone therapy can reduce the mortality rate of patients with severe coronavirus disease 2019 (COVID-19) remains controversial, and its effects on the length of hospital stay and virus shedding time are also unknown. This retrospective study investigates the previous issues to provide more evidence for methylprednisolone treatment in severe COVID-19.</p><p><strong>Methods: </strong>This retrospective study included 563 of 4827 patients with confirmed COVID-19 admitted to Wuhan Huoshenshan Hospital or Wuhan Guanggu Hospital between February 3, 2020 and March 30, 2020 who met the screening criteria. The participants' epidemiological and demographic data, comorbidities, laboratory test results, treatments, outcomes, and vital clinical time points were extracted from electronic medical records. The primary outcome was in-hospital death, and the secondary outcomes were 2 clinical courses: length from admission to viral clearance and discharge. Univariate and multivariate logistic or linear regression analyses were used to assess the role of methylprednisolone in different outcomes. Propensity score matching was performed to control for confounding factors.</p><p><strong>Results: </strong>Of the 563 patients who met the screening criteria and were included in the subsequent analysis, 138 were included in the methylprednisolone group and 425 in the nonmethylprednisolone group. The in-hospital death rate between the methylprednisolone and nonmethylprednisolone groups showed a significant difference (23.91% <i>vs.</i> 1.65%, <i>P</i> < 0.001), which was maintained after propensity score matching (13.98% <i>vs.</i> 5.38%, <i>P</i> = 0.048). However, univariate logistic analysis in the matched groups showed that methylprednisolone treatment (odds ratio [OR], 5.242; 95% confidence interval [CI], 0.802 to 34.246; <i>P</i> = 0.084) was not a risk factor for in-hospital death in severe patients. Further multivariate logistic regression analysis found comorbidities (OR, 3.327; 95% CI, 1.702 to 6.501; <i>P</i> < 0.001), lower lymphocyte count (OR, 0.076; 95% CI, 0.012 to 0.461; <i>P</i> = 0.005), higher lactate dehydrogenase (LDH) levels (OR, 1.008; 95% CI, 1.003 to 1.013; <i>P</i> = 0.002), and anticoagulation therapy (OR, 11.187; 95% CI, 2.459 to 50.900; <i>P</i> = 0.002) were associated with in-hospital mortality. Multivariate linear regression analysis in the matched groups showed that methylprednisolone treatment was not a risk factor for a prolonged duration from admission to viral clearance (β Value 0.081; 95% CI, -1.012 to 3.657; <i>P</i> = 0.265) or discharge (β Value 0.114; 95% CI, -0.723 to 6.408; <i>P</i> = 0.117). d-dimer (β Value, 0.144; 95% CI, 0.012 to 0.817; <i>P</i> = 0.044), LDH (β Value 0.260; 95% CI, 0.010 to 0.034; <i>P</i> < 0.001), and antiviral therapy (β Value 0.220; 95% CI, 1.373 to 6.263; <i>P</i> = 0.002) were associated with a longer length from admission to viral clearance. The lymphocyte count (β Value -0.206; 95% CI, -6.248 to -1.197; <i>P</i> = 0.004), LDH (β Value 0.231; 95% CI, 0.012 to 0.048; <i>P</i> = 0.001), antiviral therapy (β Value 0.143; 95% CI, 0.058 to 7.497; <i>P</i> = 0.047), and antibacterial therapy (β Value 0.152; 95% CI, 0.133 to 8.154; <i>P</i> = 0.043) were associated with a longer hospitalization duration from admission to discharge. Further stratified analysis revealed that the low daily dose group (≤60 mg/d) and the low total dose group (≤200 mg) had shorter duration from admission to viral clearance (Z=-2.362, <i>P</i> = 0.018; Z=-2.010, <i>P</i> = 0.044) and a shorter hospital stay (Z=-2.735, <i>P</i> = 0.006; Z=-3.858, <i>P</i> < 0.001).</p><p><strong>Conclusions: </strong>In patients with severe COVID-19, methylprednisolone is safe and does not prolong the duration from admission to viral clearance or discharge. Low-dose, short-term methylprednisolone treatment may be more beneficial in shortening the disease course.</p>\",\"PeriodicalId\":73371,\"journal\":{\"name\":\"Infectious diseases & immunity\",\"volume\":\"3 1\",\"pages\":\"20-28\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/72/84/idi-3-20.PMC9912987.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious diseases & immunity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/ID9.0000000000000076\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious diseases & immunity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/ID9.0000000000000076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Effect of Methylprednisolone on Mortality and Clinical Courses in Patients with Severe COVID-19: A Propensity Score Matching Analysis.
Background: Whether methylprednisolone therapy can reduce the mortality rate of patients with severe coronavirus disease 2019 (COVID-19) remains controversial, and its effects on the length of hospital stay and virus shedding time are also unknown. This retrospective study investigates the previous issues to provide more evidence for methylprednisolone treatment in severe COVID-19.
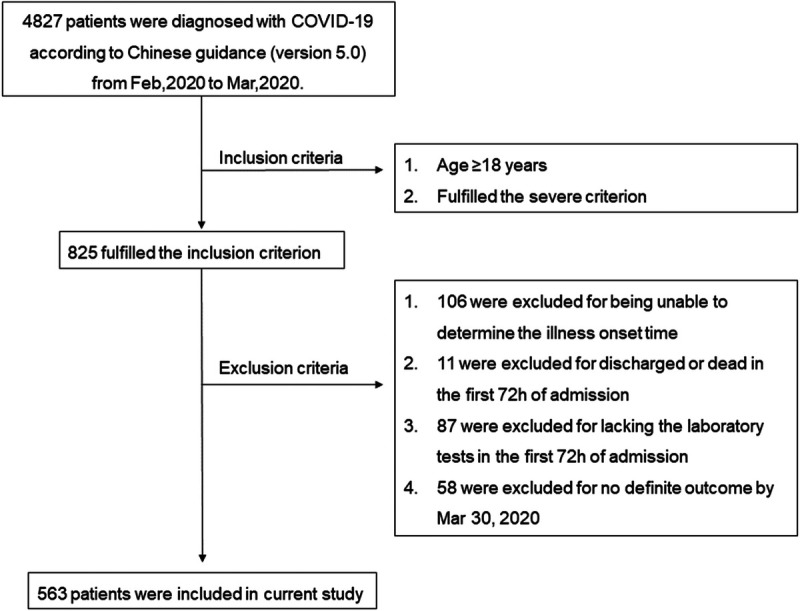
Methods: This retrospective study included 563 of 4827 patients with confirmed COVID-19 admitted to Wuhan Huoshenshan Hospital or Wuhan Guanggu Hospital between February 3, 2020 and March 30, 2020 who met the screening criteria. The participants' epidemiological and demographic data, comorbidities, laboratory test results, treatments, outcomes, and vital clinical time points were extracted from electronic medical records. The primary outcome was in-hospital death, and the secondary outcomes were 2 clinical courses: length from admission to viral clearance and discharge. Univariate and multivariate logistic or linear regression analyses were used to assess the role of methylprednisolone in different outcomes. Propensity score matching was performed to control for confounding factors.
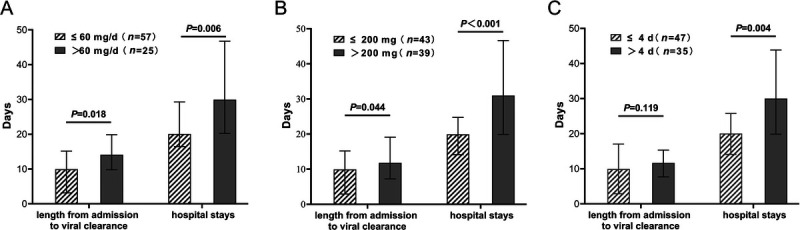
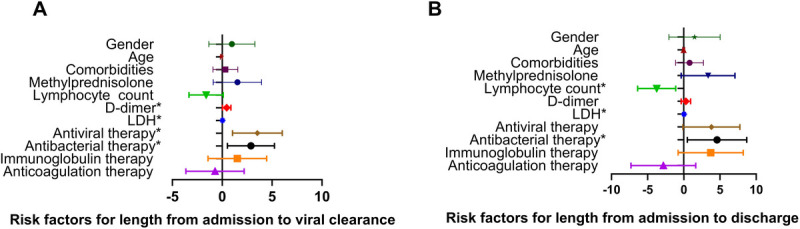
Results: Of the 563 patients who met the screening criteria and were included in the subsequent analysis, 138 were included in the methylprednisolone group and 425 in the nonmethylprednisolone group. The in-hospital death rate between the methylprednisolone and nonmethylprednisolone groups showed a significant difference (23.91% vs. 1.65%, P < 0.001), which was maintained after propensity score matching (13.98% vs. 5.38%, P = 0.048). However, univariate logistic analysis in the matched groups showed that methylprednisolone treatment (odds ratio [OR], 5.242; 95% confidence interval [CI], 0.802 to 34.246; P = 0.084) was not a risk factor for in-hospital death in severe patients. Further multivariate logistic regression analysis found comorbidities (OR, 3.327; 95% CI, 1.702 to 6.501; P < 0.001), lower lymphocyte count (OR, 0.076; 95% CI, 0.012 to 0.461; P = 0.005), higher lactate dehydrogenase (LDH) levels (OR, 1.008; 95% CI, 1.003 to 1.013; P = 0.002), and anticoagulation therapy (OR, 11.187; 95% CI, 2.459 to 50.900; P = 0.002) were associated with in-hospital mortality. Multivariate linear regression analysis in the matched groups showed that methylprednisolone treatment was not a risk factor for a prolonged duration from admission to viral clearance (β Value 0.081; 95% CI, -1.012 to 3.657; P = 0.265) or discharge (β Value 0.114; 95% CI, -0.723 to 6.408; P = 0.117). d-dimer (β Value, 0.144; 95% CI, 0.012 to 0.817; P = 0.044), LDH (β Value 0.260; 95% CI, 0.010 to 0.034; P < 0.001), and antiviral therapy (β Value 0.220; 95% CI, 1.373 to 6.263; P = 0.002) were associated with a longer length from admission to viral clearance. The lymphocyte count (β Value -0.206; 95% CI, -6.248 to -1.197; P = 0.004), LDH (β Value 0.231; 95% CI, 0.012 to 0.048; P = 0.001), antiviral therapy (β Value 0.143; 95% CI, 0.058 to 7.497; P = 0.047), and antibacterial therapy (β Value 0.152; 95% CI, 0.133 to 8.154; P = 0.043) were associated with a longer hospitalization duration from admission to discharge. Further stratified analysis revealed that the low daily dose group (≤60 mg/d) and the low total dose group (≤200 mg) had shorter duration from admission to viral clearance (Z=-2.362, P = 0.018; Z=-2.010, P = 0.044) and a shorter hospital stay (Z=-2.735, P = 0.006; Z=-3.858, P < 0.001).
Conclusions: In patients with severe COVID-19, methylprednisolone is safe and does not prolong the duration from admission to viral clearance or discharge. Low-dose, short-term methylprednisolone treatment may be more beneficial in shortening the disease course.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
