Jiyeon Song, Jae Yeong Cho, Kye Hun Kim, Ga Hui Choi, Nuri Lee, Hyung Yoon Kim, Hyukjin Park, Hyun Ju Yoon, Ju Han Kim, Youngkeun Ahn, Myung Ho Jeong, Jeong Gwan Cho
{"title":"持续性心房颤动患者三尖瓣反流进展的预测因素。","authors":"Jiyeon Song, Jae Yeong Cho, Kye Hun Kim, Ga Hui Choi, Nuri Lee, Hyung Yoon Kim, Hyukjin Park, Hyun Ju Yoon, Ju Han Kim, Youngkeun Ahn, Myung Ho Jeong, Jeong Gwan Cho","doi":"10.4068/cmj.2023.59.1.70","DOIUrl":null,"url":null,"abstract":"<p><p>Previous studies have shown that tricuspid regurgitation (TR) can be developed in patients with atrial fibrillation (AF) due to annular dilatation. This study aimed to investigate the incidence and predictors of the progression of TR in patients with persistent AF. A total of 397 patients (66.9±11.4 years, 247 men; 62.2%) with persistent AF were enrolled between 2006 and 2016 in a tertiary hospital, and 287 eligible patients with follow-up echocardiography were analyzed. They were divided into two groups according to TR progression (progression group [n=68, 70.1±10.7 years, 48.5% men] vs. non-progression group [n=219, 66.0±11.3 years, 64.8% men]). Among 287 patients in the analysis, 68 had worsening TR severity (23.7%). Patients in the TR progression group were older and more likely to be female. Patients with left ventricular ejection fraction <50% were less frequent in the progression group than those in the non-progression group (7.4% vs. 19.6%, p=0.018). Patients with mitral valve disease were more frequent in the progression group. Multivariate analysis with COX regression demonstrated independent predictors of TR progression, including left atrial (LA) diameter >54 mm (HR 4.85, 95%CI 2.23-10.57, p<0.001), E/e' (HR 1.05, 95%CI 1.01-1.10, p=0.027), and no use of antiarrhythmic agents (HR 2.20, 95%CI 1.03-4.72, p=0.041). In patients with persistent AF, worsening TR was not uncommon. The independent predictors of TR progression turned out to be greater LA diameter, higher E/e', and no use of antiarrhythmic agents.</p>","PeriodicalId":10307,"journal":{"name":"Chonnam Medical Journal","volume":"59 1","pages":"70-75"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ee/74/cmj-59-70.PMC9900221.pdf","citationCount":"1","resultStr":"{\"title\":\"Predictors of Progression of Tricuspid Regurgitation in Patients with Persistent Atrial Fibrillation.\",\"authors\":\"Jiyeon Song, Jae Yeong Cho, Kye Hun Kim, Ga Hui Choi, Nuri Lee, Hyung Yoon Kim, Hyukjin Park, Hyun Ju Yoon, Ju Han Kim, Youngkeun Ahn, Myung Ho Jeong, Jeong Gwan Cho\",\"doi\":\"10.4068/cmj.2023.59.1.70\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Previous studies have shown that tricuspid regurgitation (TR) can be developed in patients with atrial fibrillation (AF) due to annular dilatation. This study aimed to investigate the incidence and predictors of the progression of TR in patients with persistent AF. A total of 397 patients (66.9±11.4 years, 247 men; 62.2%) with persistent AF were enrolled between 2006 and 2016 in a tertiary hospital, and 287 eligible patients with follow-up echocardiography were analyzed. They were divided into two groups according to TR progression (progression group [n=68, 70.1±10.7 years, 48.5% men] vs. non-progression group [n=219, 66.0±11.3 years, 64.8% men]). Among 287 patients in the analysis, 68 had worsening TR severity (23.7%). Patients in the TR progression group were older and more likely to be female. Patients with left ventricular ejection fraction <50% were less frequent in the progression group than those in the non-progression group (7.4% vs. 19.6%, p=0.018). Patients with mitral valve disease were more frequent in the progression group. Multivariate analysis with COX regression demonstrated independent predictors of TR progression, including left atrial (LA) diameter >54 mm (HR 4.85, 95%CI 2.23-10.57, p<0.001), E/e' (HR 1.05, 95%CI 1.01-1.10, p=0.027), and no use of antiarrhythmic agents (HR 2.20, 95%CI 1.03-4.72, p=0.041). In patients with persistent AF, worsening TR was not uncommon. The independent predictors of TR progression turned out to be greater LA diameter, higher E/e', and no use of antiarrhythmic agents.</p>\",\"PeriodicalId\":10307,\"journal\":{\"name\":\"Chonnam Medical Journal\",\"volume\":\"59 1\",\"pages\":\"70-75\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ee/74/cmj-59-70.PMC9900221.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chonnam Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4068/cmj.2023.59.1.70\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chonnam Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4068/cmj.2023.59.1.70","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
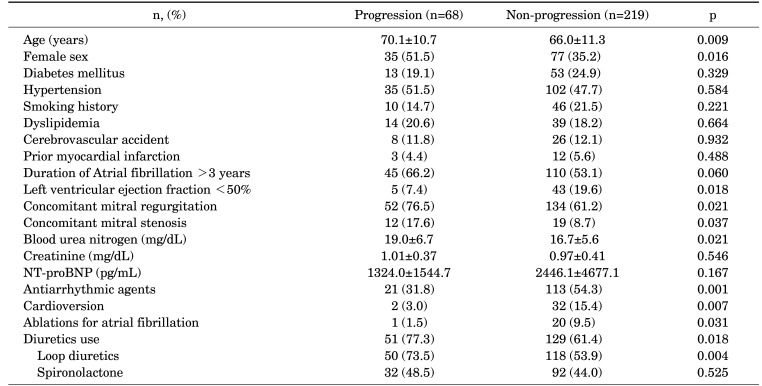
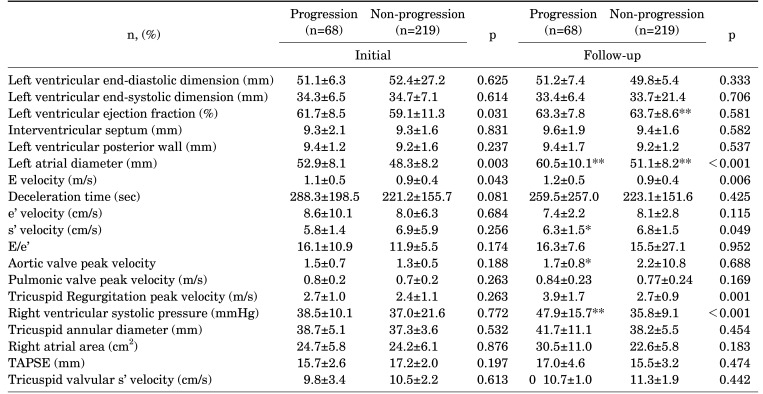
既往研究表明心房颤动(AF)患者由于心房环扩张可发生三尖瓣反流(TR)。本研究旨在探讨持续性房颤患者TR进展的发生率和预测因素。共有397例患者(66.9±11.4年,247例男性;2006 - 2016年,62.2%的患者入组于某三级医院,随访超声心动图分析287例符合条件的患者。根据TR进展情况分为两组(进展组[n=68, 70.1±10.7年,48.5%男性]和非进展组[n=219, 66.0±11.3年,64.8%男性])。在分析的287例患者中,68例TR严重程度加重(23.7%)。TR进展组患者年龄较大,女性居多。左室射血分数54 mm的患者(HR 4.85, 95%CI 2.23-10.57, p
Predictors of Progression of Tricuspid Regurgitation in Patients with Persistent Atrial Fibrillation.
Previous studies have shown that tricuspid regurgitation (TR) can be developed in patients with atrial fibrillation (AF) due to annular dilatation. This study aimed to investigate the incidence and predictors of the progression of TR in patients with persistent AF. A total of 397 patients (66.9±11.4 years, 247 men; 62.2%) with persistent AF were enrolled between 2006 and 2016 in a tertiary hospital, and 287 eligible patients with follow-up echocardiography were analyzed. They were divided into two groups according to TR progression (progression group [n=68, 70.1±10.7 years, 48.5% men] vs. non-progression group [n=219, 66.0±11.3 years, 64.8% men]). Among 287 patients in the analysis, 68 had worsening TR severity (23.7%). Patients in the TR progression group were older and more likely to be female. Patients with left ventricular ejection fraction <50% were less frequent in the progression group than those in the non-progression group (7.4% vs. 19.6%, p=0.018). Patients with mitral valve disease were more frequent in the progression group. Multivariate analysis with COX regression demonstrated independent predictors of TR progression, including left atrial (LA) diameter >54 mm (HR 4.85, 95%CI 2.23-10.57, p<0.001), E/e' (HR 1.05, 95%CI 1.01-1.10, p=0.027), and no use of antiarrhythmic agents (HR 2.20, 95%CI 1.03-4.72, p=0.041). In patients with persistent AF, worsening TR was not uncommon. The independent predictors of TR progression turned out to be greater LA diameter, higher E/e', and no use of antiarrhythmic agents.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
