Meredith E Mowitz, Wei Gao, Heather Sipsma, Pete Zuckerman, Hallee Wong, Rajeev Ayyagari, Sujata P Sarda
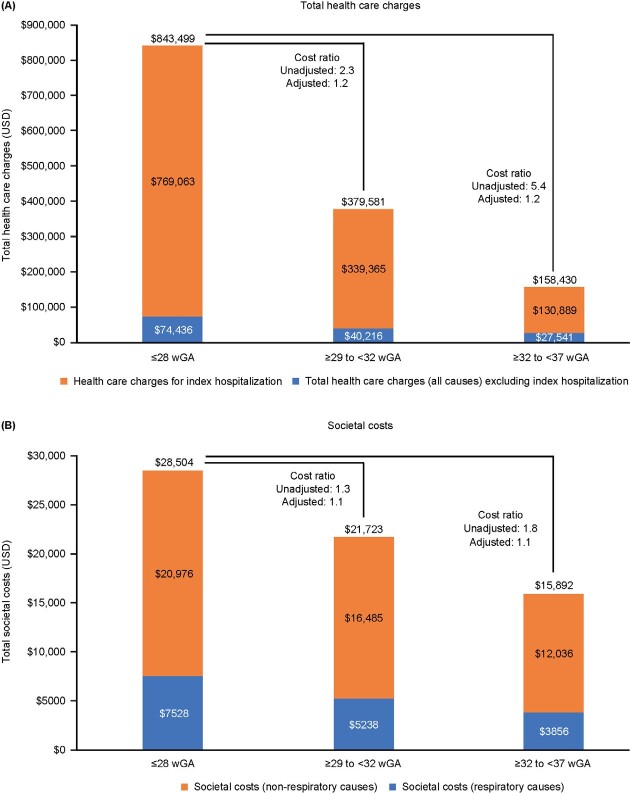
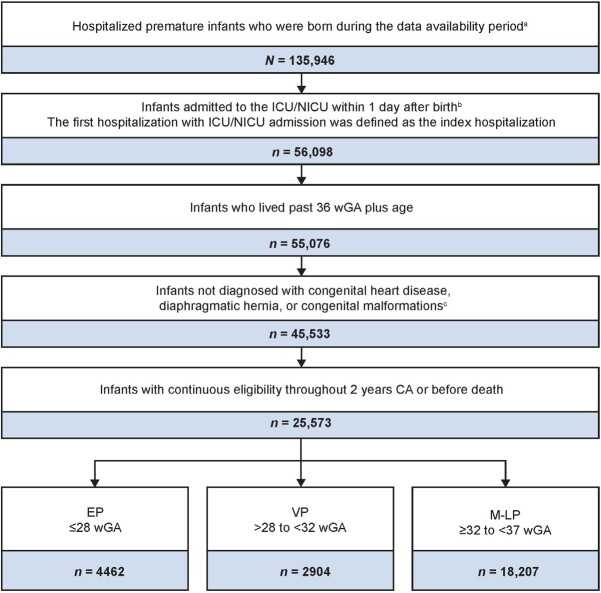
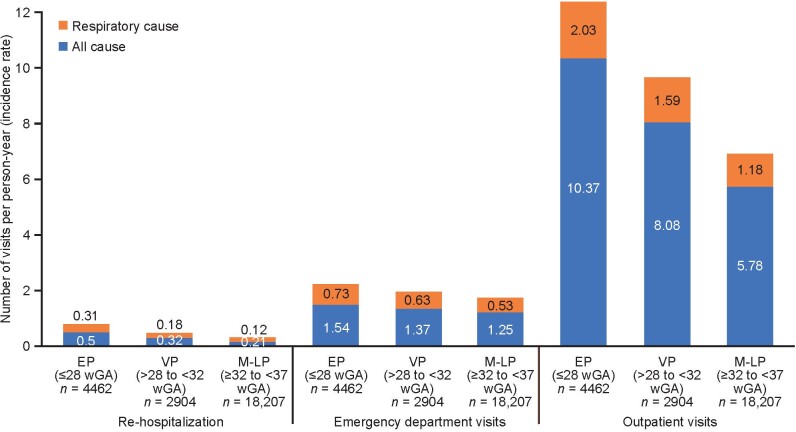
{"title":"参保极早产儿的合并症负担与医疗资源利用","authors":"Meredith E Mowitz, Wei Gao, Heather Sipsma, Pete Zuckerman, Hallee Wong, Rajeev Ayyagari, Sujata P Sarda","doi":"10.36469/001c.38847","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The effect of gestational age (GA) on comorbidity prevalence, healthcare resource utilization (HCRU), and all-cause costs is significant for extremely premature (EP) infants in the United States. <b>Objectives:</b> To characterize real-world patient characteristics, prevalence of comorbidities, rates of HCRU, and direct healthcare charges and societal costs among premature infants in US Medicaid programs, with respect to GA and the presence of respiratory comorbidities. <b>Methods:</b> Using <i>International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification</i> codes, diagnosis and medical claims data from 6 state Medicaid databases (1997-2018) of infants born at less than 37 weeks of GA (wGA) were collected retrospectively. Data from the index date (birth) up to 2 years corrected age or death, stratified by GA (EP, ≤28 wGA; very premature [VP], >28 to <32 wGA; and moderate to late premature [M-LP], ≥32 to <37 wGA), were compared using unadjusted and adjusted generalized linear models. <b>Results:</b> Among 25 573 premature infants (46.1% female; 4462 [17.4%] EP; 2904 [11.4%] VP; 18 207 [71.2%] M-LP), comorbidity prevalence, HCRU, and all-cause costs increased with decreasing GA and were highest for EP. Total healthcare charges, excluding index hospitalization and all-cause societal costs (US dollars), were 2 to 3 times higher for EP than for M-LP (EP $74 436 vs M-LP $27 541 and EP $28 504 vs M-LP $15 892, respectively). <b>Conclusions:</b> Complications of preterm birth, including prevalence of comorbidities, HCRU, and costs, increased with decreasing GA and were highest among EP infants during the first 2 years in this US analysis.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"9 2","pages":"147-155"},"PeriodicalIF":2.3000,"publicationDate":"2022-12-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9790150/pdf/","citationCount":"0","resultStr":"{\"title\":\"Burden of Comorbidities and Healthcare Resource Utilization Among Medicaid-Enrolled Extremely Premature Infants.\",\"authors\":\"Meredith E Mowitz, Wei Gao, Heather Sipsma, Pete Zuckerman, Hallee Wong, Rajeev Ayyagari, Sujata P Sarda\",\"doi\":\"10.36469/001c.38847\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> The effect of gestational age (GA) on comorbidity prevalence, healthcare resource utilization (HCRU), and all-cause costs is significant for extremely premature (EP) infants in the United States. <b>Objectives:</b> To characterize real-world patient characteristics, prevalence of comorbidities, rates of HCRU, and direct healthcare charges and societal costs among premature infants in US Medicaid programs, with respect to GA and the presence of respiratory comorbidities. <b>Methods:</b> Using <i>International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification</i> codes, diagnosis and medical claims data from 6 state Medicaid databases (1997-2018) of infants born at less than 37 weeks of GA (wGA) were collected retrospectively. Data from the index date (birth) up to 2 years corrected age or death, stratified by GA (EP, ≤28 wGA; very premature [VP], >28 to <32 wGA; and moderate to late premature [M-LP], ≥32 to <37 wGA), were compared using unadjusted and adjusted generalized linear models. <b>Results:</b> Among 25 573 premature infants (46.1% female; 4462 [17.4%] EP; 2904 [11.4%] VP; 18 207 [71.2%] M-LP), comorbidity prevalence, HCRU, and all-cause costs increased with decreasing GA and were highest for EP. Total healthcare charges, excluding index hospitalization and all-cause societal costs (US dollars), were 2 to 3 times higher for EP than for M-LP (EP $74 436 vs M-LP $27 541 and EP $28 504 vs M-LP $15 892, respectively). <b>Conclusions:</b> Complications of preterm birth, including prevalence of comorbidities, HCRU, and costs, increased with decreasing GA and were highest among EP infants during the first 2 years in this US analysis.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"9 2\",\"pages\":\"147-155\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-12-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9790150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36469/001c.38847\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.38847","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:在美国,胎龄(GA)对极早产儿(EP)的共病患病率、医疗资源利用率(HCRU)和全因成本的影响是显著的。目的:描述美国医疗补助计划中早产儿的真实患者特征、合并症的患病率、HCRU的发生率、直接医疗费用和社会成本,以及GA和呼吸合并症的存在。方法:使用《国际疾病分类》第九/第十版、临床修改代码、6个州医疗补助数据库(1997-2018年)中小于37周出生婴儿(wGA)的诊断和医疗索赔数据进行回顾性收集。数据从指标日期(出生)到2岁校正年龄或死亡,按GA分层(EP,≤28 wGA;结果:25573例早产儿中,女性占46.1%;4462 [17.4%] ep;2904 [11.4%] vp;18 207 [71.2%]M-LP),合并症患病率,HCRU和全因成本随着GA的降低而增加,EP最高。不包括指数住院和全因社会成本(美元),EP的总医疗费用比M-LP高2至3倍(EP 74美元 436 vs M-LP 27美元 541,EP 28美元 504 vs M-LP 15美元 892)。结论:早产的并发症,包括合并症的患病率、HCRU和成本,随着GA的降低而增加,并且在前2年EP婴儿中最高。
Burden of Comorbidities and Healthcare Resource Utilization Among Medicaid-Enrolled Extremely Premature Infants.
Background: The effect of gestational age (GA) on comorbidity prevalence, healthcare resource utilization (HCRU), and all-cause costs is significant for extremely premature (EP) infants in the United States. Objectives: To characterize real-world patient characteristics, prevalence of comorbidities, rates of HCRU, and direct healthcare charges and societal costs among premature infants in US Medicaid programs, with respect to GA and the presence of respiratory comorbidities. Methods: Using International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification codes, diagnosis and medical claims data from 6 state Medicaid databases (1997-2018) of infants born at less than 37 weeks of GA (wGA) were collected retrospectively. Data from the index date (birth) up to 2 years corrected age or death, stratified by GA (EP, ≤28 wGA; very premature [VP], >28 to <32 wGA; and moderate to late premature [M-LP], ≥32 to <37 wGA), were compared using unadjusted and adjusted generalized linear models. Results: Among 25 573 premature infants (46.1% female; 4462 [17.4%] EP; 2904 [11.4%] VP; 18 207 [71.2%] M-LP), comorbidity prevalence, HCRU, and all-cause costs increased with decreasing GA and were highest for EP. Total healthcare charges, excluding index hospitalization and all-cause societal costs (US dollars), were 2 to 3 times higher for EP than for M-LP (EP $74 436 vs M-LP $27 541 and EP $28 504 vs M-LP $15 892, respectively). Conclusions: Complications of preterm birth, including prevalence of comorbidities, HCRU, and costs, increased with decreasing GA and were highest among EP infants during the first 2 years in this US analysis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
