{"title":"治疗的必要性、住院治疗之外的另一种限制性较小的治疗方法以及治疗的提供:社区治疗令的效用。","authors":"Steven P Segal, Lachlan Rimes, Leena Badran","doi":"10.1093/schizbullopen/sgac071","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Provision of involuntary care is an abridgment of civil rights and a source of controversy. Its circumstances require continued monitoring. This study asks 4 questions: Whether, in an era, focused on allowing patients with capacity to refuse community-treatment-order (CTO)-assignments, CTO use decreased. And whether CTOs fulfilled 3 statute mandates: Were CTO-assigned patients in greater need of treatment than other psychiatric inpatients? Was CTO assignment a less-restrictive alternative to psychiatric hospitalization? and Did CTO assignment provide needed treatment at internationally recommended levels with consequences for patient outcomes?</p><p><strong>Method: </strong>All 214 388 Victoria, Australia mental health admissions between 2000- 2017 were reviewed. Two cohort samples were drawn and followed through 2019-ie, all 7826 hospitalized patients who were first placed on CTOs from 2010 to 2017 and 13 896 hospitalized patients without CTO placement. Logistic Regression was used to specify determinants of CTO assignment from the psychiatric inpatient population. OLS Regression with propensity score control to evaluate study questions.</p><p><strong>Results: </strong>In the 2010-2017 decade, initial CTO assignments decreased by 3.5%, and initial hospitalizations increased by 5.9% compared to the 2000-2009 period. At hospital admission and discharge, based on Health of the Nations Score ratings, the CTO-cohort's need for treatment exceeded that of non-CTO patients. CTO patients had 3.75 fewer days in average inpatient episode duration than other inpatients, when adjusted for CTO-assignment determinants, the ratio of patients to community case managers, and patient housing status. CTO patients needing rehospitalization spent 112.68 more days in the community than re-hospitalized non-CTO patients. Patient to case-manager ratios falling above recommended levels and the patient marginal housing status contributed to longer hospital stays and reduced community tenure.</p><p><strong>Conclusions: </strong>Victoria relied less on CTOs as an LRA, consequently, experiencing increased initial hospitalizations. CTO patients were in greater need of treatment than non-CTO patients, yet, with required oversite had shorter hospitalizations and more time out of hospital prior to rehospitalization than the less severely ill non-CTO group. Patient LRA outcomes were adversely affected by higher than recommended community patient to case-manager ratios limiting needed treatment provision to hospital.</p>","PeriodicalId":21348,"journal":{"name":"Schizophrenia Bulletin Open","volume":"4 1","pages":"sgac071"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/cc/sgac071.PMC9894024.pdf","citationCount":"0","resultStr":"{\"title\":\"Need for Treatment, A Less Restrictive Alternative to Hospitalization, and Treatment Provision: The Utility of Community Treatment Orders.\",\"authors\":\"Steven P Segal, Lachlan Rimes, Leena Badran\",\"doi\":\"10.1093/schizbullopen/sgac071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Provision of involuntary care is an abridgment of civil rights and a source of controversy. Its circumstances require continued monitoring. This study asks 4 questions: Whether, in an era, focused on allowing patients with capacity to refuse community-treatment-order (CTO)-assignments, CTO use decreased. And whether CTOs fulfilled 3 statute mandates: Were CTO-assigned patients in greater need of treatment than other psychiatric inpatients? Was CTO assignment a less-restrictive alternative to psychiatric hospitalization? and Did CTO assignment provide needed treatment at internationally recommended levels with consequences for patient outcomes?</p><p><strong>Method: </strong>All 214 388 Victoria, Australia mental health admissions between 2000- 2017 were reviewed. Two cohort samples were drawn and followed through 2019-ie, all 7826 hospitalized patients who were first placed on CTOs from 2010 to 2017 and 13 896 hospitalized patients without CTO placement. Logistic Regression was used to specify determinants of CTO assignment from the psychiatric inpatient population. OLS Regression with propensity score control to evaluate study questions.</p><p><strong>Results: </strong>In the 2010-2017 decade, initial CTO assignments decreased by 3.5%, and initial hospitalizations increased by 5.9% compared to the 2000-2009 period. At hospital admission and discharge, based on Health of the Nations Score ratings, the CTO-cohort's need for treatment exceeded that of non-CTO patients. CTO patients had 3.75 fewer days in average inpatient episode duration than other inpatients, when adjusted for CTO-assignment determinants, the ratio of patients to community case managers, and patient housing status. CTO patients needing rehospitalization spent 112.68 more days in the community than re-hospitalized non-CTO patients. Patient to case-manager ratios falling above recommended levels and the patient marginal housing status contributed to longer hospital stays and reduced community tenure.</p><p><strong>Conclusions: </strong>Victoria relied less on CTOs as an LRA, consequently, experiencing increased initial hospitalizations. CTO patients were in greater need of treatment than non-CTO patients, yet, with required oversite had shorter hospitalizations and more time out of hospital prior to rehospitalization than the less severely ill non-CTO group. Patient LRA outcomes were adversely affected by higher than recommended community patient to case-manager ratios limiting needed treatment provision to hospital.</p>\",\"PeriodicalId\":21348,\"journal\":{\"name\":\"Schizophrenia Bulletin Open\",\"volume\":\"4 1\",\"pages\":\"sgac071\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/cc/sgac071.PMC9894024.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Schizophrenia Bulletin Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/schizbullopen/sgac071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Schizophrenia Bulletin Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/schizbullopen/sgac071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Need for Treatment, A Less Restrictive Alternative to Hospitalization, and Treatment Provision: The Utility of Community Treatment Orders.
Background: Provision of involuntary care is an abridgment of civil rights and a source of controversy. Its circumstances require continued monitoring. This study asks 4 questions: Whether, in an era, focused on allowing patients with capacity to refuse community-treatment-order (CTO)-assignments, CTO use decreased. And whether CTOs fulfilled 3 statute mandates: Were CTO-assigned patients in greater need of treatment than other psychiatric inpatients? Was CTO assignment a less-restrictive alternative to psychiatric hospitalization? and Did CTO assignment provide needed treatment at internationally recommended levels with consequences for patient outcomes?
Method: All 214 388 Victoria, Australia mental health admissions between 2000- 2017 were reviewed. Two cohort samples were drawn and followed through 2019-ie, all 7826 hospitalized patients who were first placed on CTOs from 2010 to 2017 and 13 896 hospitalized patients without CTO placement. Logistic Regression was used to specify determinants of CTO assignment from the psychiatric inpatient population. OLS Regression with propensity score control to evaluate study questions.
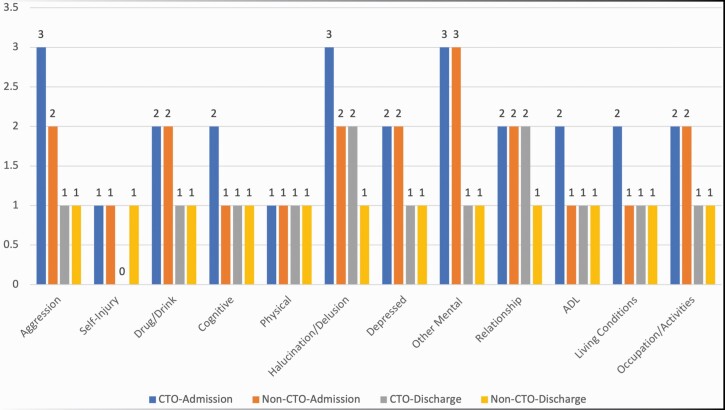
Results: In the 2010-2017 decade, initial CTO assignments decreased by 3.5%, and initial hospitalizations increased by 5.9% compared to the 2000-2009 period. At hospital admission and discharge, based on Health of the Nations Score ratings, the CTO-cohort's need for treatment exceeded that of non-CTO patients. CTO patients had 3.75 fewer days in average inpatient episode duration than other inpatients, when adjusted for CTO-assignment determinants, the ratio of patients to community case managers, and patient housing status. CTO patients needing rehospitalization spent 112.68 more days in the community than re-hospitalized non-CTO patients. Patient to case-manager ratios falling above recommended levels and the patient marginal housing status contributed to longer hospital stays and reduced community tenure.
Conclusions: Victoria relied less on CTOs as an LRA, consequently, experiencing increased initial hospitalizations. CTO patients were in greater need of treatment than non-CTO patients, yet, with required oversite had shorter hospitalizations and more time out of hospital prior to rehospitalization than the less severely ill non-CTO group. Patient LRA outcomes were adversely affected by higher than recommended community patient to case-manager ratios limiting needed treatment provision to hospital.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
