Vykuntaraju K Gowda, Balamurugan Natarajan, Varunvenkat M Srinivasan, Sanjay K Shivappa
{"title":"可治疗的神经退行性疾病:脑叶酸运输缺乏症——来自印度南部的两个孩子。","authors":"Vykuntaraju K Gowda, Balamurugan Natarajan, Varunvenkat M Srinivasan, Sanjay K Shivappa","doi":"10.4103/jpn.JPN_76_20","DOIUrl":null,"url":null,"abstract":"<p><p>Cerebral folate transport deficiency results from impaired folate transport across the blood:choroid plexus:cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate (5MTHF), the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Case 1: Seventeen-year-old boy presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had pyramidal and cerebellar signs. Magnetic resonance imaging (MRI) of brain revealed diffuse cerebral and cerebellar atrophy. Targeted next generation sequencing revealed homozygous missense pathogenic variant in <i>FOLR1</i> gene in exon 4 c.382C>T p.R128W, confirming the diagnosis of cerebral folate deficiency. Case 2: Six-year-old male child presented with delayed milestones, myoclonic jerks and cognitive regression from 3 years of age. Child had microcephaly with ataxia. Computed tomography (CT) of brain revealed multifocal calcifications. MRI brain revealed cerebellar atrophy with hyperintense T2 signal changes in the subcortical white matter of frontal and temporal lobes. Genetic testing revealed homozygous variant (c.493+2_493+6delTGAGG) in intron 4 of the <i>FOLR1</i> gene which is a novel pathogenic variant. Both children started on folinic acid and there was a significant improvement in development, behavior, ataxia, and decrease in seizure frequency. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, epilepsy, ataxia and neuroimaging showing cerebellar atrophy and calcification. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.</p>","PeriodicalId":46746,"journal":{"name":"Journal of Pediatric Neurosciences","volume":"16 4","pages":"273-276"},"PeriodicalIF":0.2000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9757528/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatable Neurodegenerative Disorder: Cerebral Folate Transport Deficiency--Two Children from Southern India.\",\"authors\":\"Vykuntaraju K Gowda, Balamurugan Natarajan, Varunvenkat M Srinivasan, Sanjay K Shivappa\",\"doi\":\"10.4103/jpn.JPN_76_20\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cerebral folate transport deficiency results from impaired folate transport across the blood:choroid plexus:cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate (5MTHF), the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Case 1: Seventeen-year-old boy presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had pyramidal and cerebellar signs. Magnetic resonance imaging (MRI) of brain revealed diffuse cerebral and cerebellar atrophy. Targeted next generation sequencing revealed homozygous missense pathogenic variant in <i>FOLR1</i> gene in exon 4 c.382C>T p.R128W, confirming the diagnosis of cerebral folate deficiency. Case 2: Six-year-old male child presented with delayed milestones, myoclonic jerks and cognitive regression from 3 years of age. Child had microcephaly with ataxia. Computed tomography (CT) of brain revealed multifocal calcifications. MRI brain revealed cerebellar atrophy with hyperintense T2 signal changes in the subcortical white matter of frontal and temporal lobes. Genetic testing revealed homozygous variant (c.493+2_493+6delTGAGG) in intron 4 of the <i>FOLR1</i> gene which is a novel pathogenic variant. Both children started on folinic acid and there was a significant improvement in development, behavior, ataxia, and decrease in seizure frequency. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, epilepsy, ataxia and neuroimaging showing cerebellar atrophy and calcification. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.</p>\",\"PeriodicalId\":46746,\"journal\":{\"name\":\"Journal of Pediatric Neurosciences\",\"volume\":\"16 4\",\"pages\":\"273-276\"},\"PeriodicalIF\":0.2000,\"publicationDate\":\"2021-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9757528/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pediatric Neurosciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jpn.JPN_76_20\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pediatric Neurosciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jpn.JPN_76_20","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Treatable Neurodegenerative Disorder: Cerebral Folate Transport Deficiency--Two Children from Southern India.
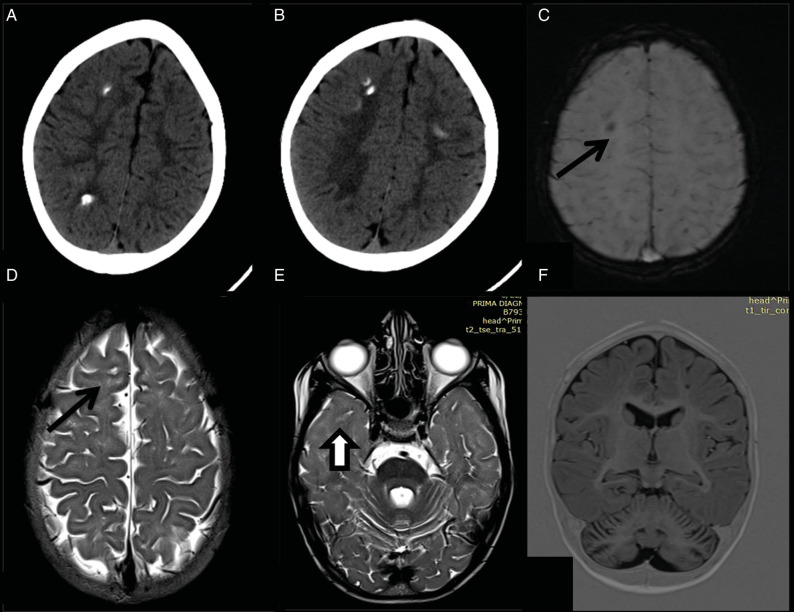
Cerebral folate transport deficiency results from impaired folate transport across the blood:choroid plexus:cerebrospinal fluid (CSF) barrier. This leads to low CSF 5-methyltetrahydrofolate (5MTHF), the active folate metabolite. We are reporting two children with this treatable cerebral folate transport deficiency. Case 1: Seventeen-year-old boy presented with delayed milestones followed by regression, seizures, and intention tremors. On examination child had pyramidal and cerebellar signs. Magnetic resonance imaging (MRI) of brain revealed diffuse cerebral and cerebellar atrophy. Targeted next generation sequencing revealed homozygous missense pathogenic variant in FOLR1 gene in exon 4 c.382C>T p.R128W, confirming the diagnosis of cerebral folate deficiency. Case 2: Six-year-old male child presented with delayed milestones, myoclonic jerks and cognitive regression from 3 years of age. Child had microcephaly with ataxia. Computed tomography (CT) of brain revealed multifocal calcifications. MRI brain revealed cerebellar atrophy with hyperintense T2 signal changes in the subcortical white matter of frontal and temporal lobes. Genetic testing revealed homozygous variant (c.493+2_493+6delTGAGG) in intron 4 of the FOLR1 gene which is a novel pathogenic variant. Both children started on folinic acid and there was a significant improvement in development, behavior, ataxia, and decrease in seizure frequency. In conclusion, cerebral folate transport deficiency should be suspected in every child with global developmental delay, epilepsy, ataxia and neuroimaging showing cerebellar atrophy and calcification. Response to folinic acid supplementation is partial if diagnosed late and treatment initiation is delayed.
期刊介绍:
Journal of Pediatric Neurosciences-JPN (ISSN 1817-1745) is official publication of the Indian Society for Pediatric Neurosurgery. The journal is published semiannually. Bibliographic listings: The journal is indexed with Caspur, DOAJ, EBSCO Publishing’s Electronic Databases, Excerpta Medica / EMBASE, Expanded Academic ASAP, Genamics JournalSeek, Google Scholar, Health & Wellness Research Center, Health Reference Center Academic, Hinari, Index Copernicus, OpenJGate, Scimago Journal Ranking, SCOLOAR, SCOPUS, SIIC databases, Ulrich’s International Periodical Directory




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
