{"title":"阿片类相关遗忘综合征进展为弥漫性脑白质病。","authors":"Dylan Meng, Jason Randhawa","doi":"10.1177/19418744211045862","DOIUrl":null,"url":null,"abstract":"A 49-year-old female with a history of polysubstance use was found unconscious. Drug screen was positive for cocaine, opioids, and fentanyl. Upon awakening, she did not recall the 24 hours prior to her presentation. She had profound anterograde amnesia with no other focal deficits. Lumbar puncture and electroencephalography were unremarkable. Brain MRI revealed restricted diffusion in both hippocampi with associated T2-weighted-Fluid-Attenuated Inversion Recovery (FLAIR) hyperintensities (Figure 1). Three weeks into admission, she developed parkinsonism progressing to akinetic mutism. Repeat MRI showed resolution of the bilateral hippocampal findings with development of diffuse T2-FLAIR white matter hyperintensities consistent with delayed leukoencephalopathy (Figure 1). She had minimal response to medical management and is currently in long-term care. Over forty cases of an acute amnestic syndrome with bilateral hippocampal imaging changes in the context of opioid use have been reported, recently termed opioid-associated amnestic syndrome (OAS). Neuroimaging findings often resolve within days to weeks of the inciting event making diagnosis challenging in this vulnerable population.We report the second case of a diffuse leukoencephalopathy occurringwithin weeks of confirmedOAS as recently defined by Barash et al. In this case, as with many cases of OAS, one cannot rule out the confounding effect of hypoxia as a cause. It is currently unknown how commonly OAS progresses in this manner given the scarcity of reported cases. Prognosis should remain guarded until patients with OAS have been stable for at least one month following presentation based on two recent cases. Further study of OAS is warranted.","PeriodicalId":46355,"journal":{"name":"Neurohospitalist","volume":"13 1","pages":"109-110"},"PeriodicalIF":0.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/17/0e/10.1177_19418744211045862.PMC9755609.pdf","citationCount":"1","resultStr":"{\"title\":\"Opioid-Associated Amnestic Syndrome Progressing to Diffuse Leukoencephalopathy.\",\"authors\":\"Dylan Meng, Jason Randhawa\",\"doi\":\"10.1177/19418744211045862\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 49-year-old female with a history of polysubstance use was found unconscious. Drug screen was positive for cocaine, opioids, and fentanyl. Upon awakening, she did not recall the 24 hours prior to her presentation. She had profound anterograde amnesia with no other focal deficits. Lumbar puncture and electroencephalography were unremarkable. Brain MRI revealed restricted diffusion in both hippocampi with associated T2-weighted-Fluid-Attenuated Inversion Recovery (FLAIR) hyperintensities (Figure 1). Three weeks into admission, she developed parkinsonism progressing to akinetic mutism. Repeat MRI showed resolution of the bilateral hippocampal findings with development of diffuse T2-FLAIR white matter hyperintensities consistent with delayed leukoencephalopathy (Figure 1). She had minimal response to medical management and is currently in long-term care. Over forty cases of an acute amnestic syndrome with bilateral hippocampal imaging changes in the context of opioid use have been reported, recently termed opioid-associated amnestic syndrome (OAS). Neuroimaging findings often resolve within days to weeks of the inciting event making diagnosis challenging in this vulnerable population.We report the second case of a diffuse leukoencephalopathy occurringwithin weeks of confirmedOAS as recently defined by Barash et al. In this case, as with many cases of OAS, one cannot rule out the confounding effect of hypoxia as a cause. It is currently unknown how commonly OAS progresses in this manner given the scarcity of reported cases. Prognosis should remain guarded until patients with OAS have been stable for at least one month following presentation based on two recent cases. Further study of OAS is warranted.\",\"PeriodicalId\":46355,\"journal\":{\"name\":\"Neurohospitalist\",\"volume\":\"13 1\",\"pages\":\"109-110\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/17/0e/10.1177_19418744211045862.PMC9755609.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurohospitalist\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/19418744211045862\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurohospitalist","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/19418744211045862","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Opioid-Associated Amnestic Syndrome Progressing to Diffuse Leukoencephalopathy.
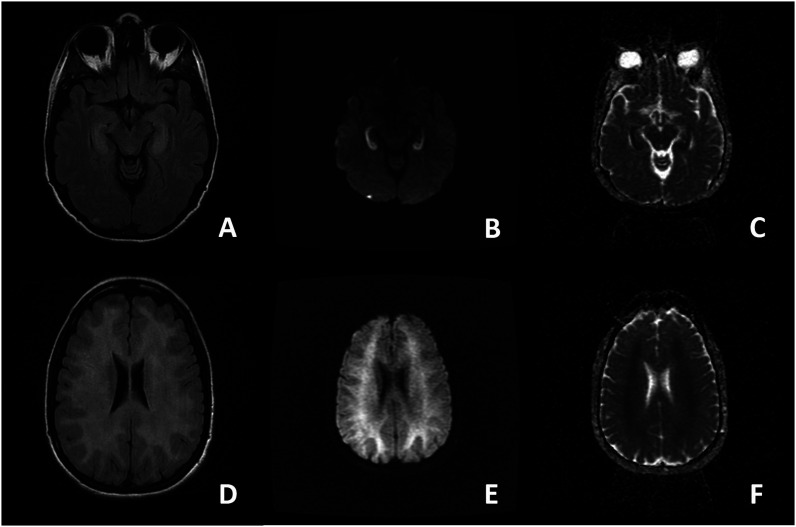
A 49-year-old female with a history of polysubstance use was found unconscious. Drug screen was positive for cocaine, opioids, and fentanyl. Upon awakening, she did not recall the 24 hours prior to her presentation. She had profound anterograde amnesia with no other focal deficits. Lumbar puncture and electroencephalography were unremarkable. Brain MRI revealed restricted diffusion in both hippocampi with associated T2-weighted-Fluid-Attenuated Inversion Recovery (FLAIR) hyperintensities (Figure 1). Three weeks into admission, she developed parkinsonism progressing to akinetic mutism. Repeat MRI showed resolution of the bilateral hippocampal findings with development of diffuse T2-FLAIR white matter hyperintensities consistent with delayed leukoencephalopathy (Figure 1). She had minimal response to medical management and is currently in long-term care. Over forty cases of an acute amnestic syndrome with bilateral hippocampal imaging changes in the context of opioid use have been reported, recently termed opioid-associated amnestic syndrome (OAS). Neuroimaging findings often resolve within days to weeks of the inciting event making diagnosis challenging in this vulnerable population.We report the second case of a diffuse leukoencephalopathy occurringwithin weeks of confirmedOAS as recently defined by Barash et al. In this case, as with many cases of OAS, one cannot rule out the confounding effect of hypoxia as a cause. It is currently unknown how commonly OAS progresses in this manner given the scarcity of reported cases. Prognosis should remain guarded until patients with OAS have been stable for at least one month following presentation based on two recent cases. Further study of OAS is warranted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
