Hyun Jin Bang, Hyun Jeong Shim, Jun Eul Hwang, Woo Kyun Bae, Ik Joo Chung, Sang Hee Cho
{"title":"临床T3-4N0直肠癌术前放化疗后辅助化疗的益处","authors":"Hyun Jin Bang, Hyun Jeong Shim, Jun Eul Hwang, Woo Kyun Bae, Ik Joo Chung, Sang Hee Cho","doi":"10.4068/cmj.2023.59.1.76","DOIUrl":null,"url":null,"abstract":"<p><p>While the guidelines for adjuvant chemotherapy (AC) for colon cancer are relatively standardized, those for early rectal cancer are still lacking. We therefore evaluated the role of AC in clinical stage II rectal cancer treatment after preoperative chemoradiotherapy (CRT). Patients diagnosed with early rectal cancer (defined by clinical stage T3/4, N0) who completed CRT followed by surgery were enrolled in this retrospective study. To evaluate the role of AC, we analyzed the risk of recurrence and survival based on clinicopathologic parameters and adjuvant chemotherapy. Of the 112 patients, 11 patients (9.8%) experienced recurrence and five patients (4.8%) died. In a multivariate analysis, circumferential resection margin involvement (CRM+) on magnetic resonance imaging at diagnosis, CRM involvement following neoadjuvant therapy (ypCRM+), tumor regression grade (≤G1) and no-AC were considered poor prognostic factors for recurrence free survival (RFS). In addition, ypCRM+ and no-AC were associated with poor overall survival (OS) in the multivariate analysis. AC including 5-FU monotherapy demonstrated the benefits of reduced recurrence and prolonged survival in clinical stage II rectal cancer, even in pathologic stage following neoadjuvant therapy (ypStage) 0-I. Further prospective studies are needed to verify the benefit of each regimen of AC and the development of a method that can accurately predict CRM status before surgery, and a vigorous treatment that can induce CRM non-involvement (CRM-) should be considered even in early stages of rectal cancer.</p>","PeriodicalId":10307,"journal":{"name":"Chonnam Medical Journal","volume":"59 1","pages":"76-82"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/14/cmj-59-76.PMC9900219.pdf","citationCount":"1","resultStr":"{\"title\":\"Benefits of Adjuvant Chemotherapy for Clinical T3-4N0 Rectal Cancer After Preoperative Chemoradiotherapy.\",\"authors\":\"Hyun Jin Bang, Hyun Jeong Shim, Jun Eul Hwang, Woo Kyun Bae, Ik Joo Chung, Sang Hee Cho\",\"doi\":\"10.4068/cmj.2023.59.1.76\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>While the guidelines for adjuvant chemotherapy (AC) for colon cancer are relatively standardized, those for early rectal cancer are still lacking. We therefore evaluated the role of AC in clinical stage II rectal cancer treatment after preoperative chemoradiotherapy (CRT). Patients diagnosed with early rectal cancer (defined by clinical stage T3/4, N0) who completed CRT followed by surgery were enrolled in this retrospective study. To evaluate the role of AC, we analyzed the risk of recurrence and survival based on clinicopathologic parameters and adjuvant chemotherapy. Of the 112 patients, 11 patients (9.8%) experienced recurrence and five patients (4.8%) died. In a multivariate analysis, circumferential resection margin involvement (CRM+) on magnetic resonance imaging at diagnosis, CRM involvement following neoadjuvant therapy (ypCRM+), tumor regression grade (≤G1) and no-AC were considered poor prognostic factors for recurrence free survival (RFS). In addition, ypCRM+ and no-AC were associated with poor overall survival (OS) in the multivariate analysis. AC including 5-FU monotherapy demonstrated the benefits of reduced recurrence and prolonged survival in clinical stage II rectal cancer, even in pathologic stage following neoadjuvant therapy (ypStage) 0-I. Further prospective studies are needed to verify the benefit of each regimen of AC and the development of a method that can accurately predict CRM status before surgery, and a vigorous treatment that can induce CRM non-involvement (CRM-) should be considered even in early stages of rectal cancer.</p>\",\"PeriodicalId\":10307,\"journal\":{\"name\":\"Chonnam Medical Journal\",\"volume\":\"59 1\",\"pages\":\"76-82\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/14/14/cmj-59-76.PMC9900219.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chonnam Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4068/cmj.2023.59.1.76\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chonnam Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4068/cmj.2023.59.1.76","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Benefits of Adjuvant Chemotherapy for Clinical T3-4N0 Rectal Cancer After Preoperative Chemoradiotherapy.
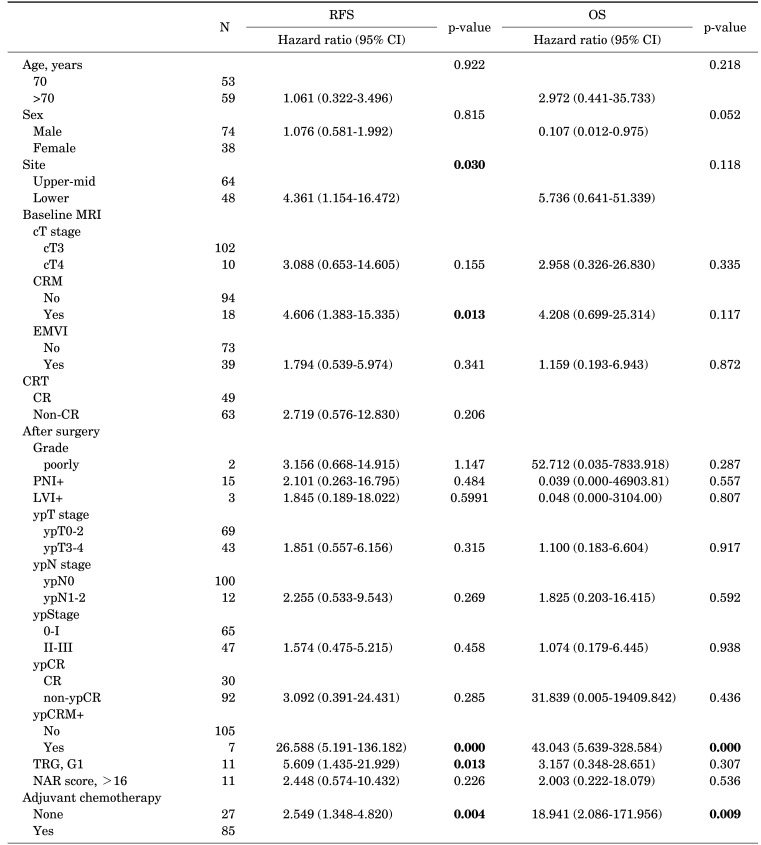
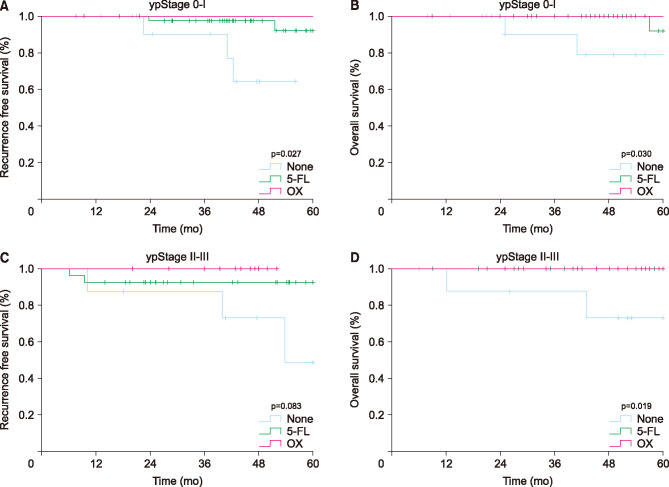
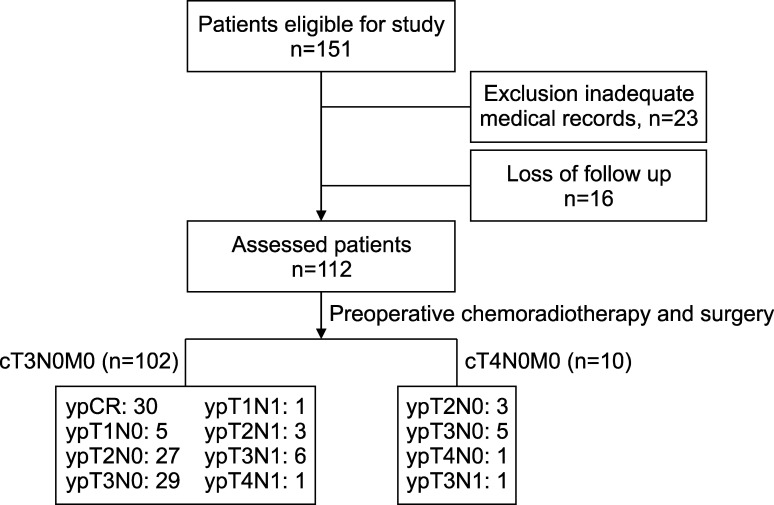
While the guidelines for adjuvant chemotherapy (AC) for colon cancer are relatively standardized, those for early rectal cancer are still lacking. We therefore evaluated the role of AC in clinical stage II rectal cancer treatment after preoperative chemoradiotherapy (CRT). Patients diagnosed with early rectal cancer (defined by clinical stage T3/4, N0) who completed CRT followed by surgery were enrolled in this retrospective study. To evaluate the role of AC, we analyzed the risk of recurrence and survival based on clinicopathologic parameters and adjuvant chemotherapy. Of the 112 patients, 11 patients (9.8%) experienced recurrence and five patients (4.8%) died. In a multivariate analysis, circumferential resection margin involvement (CRM+) on magnetic resonance imaging at diagnosis, CRM involvement following neoadjuvant therapy (ypCRM+), tumor regression grade (≤G1) and no-AC were considered poor prognostic factors for recurrence free survival (RFS). In addition, ypCRM+ and no-AC were associated with poor overall survival (OS) in the multivariate analysis. AC including 5-FU monotherapy demonstrated the benefits of reduced recurrence and prolonged survival in clinical stage II rectal cancer, even in pathologic stage following neoadjuvant therapy (ypStage) 0-I. Further prospective studies are needed to verify the benefit of each regimen of AC and the development of a method that can accurately predict CRM status before surgery, and a vigorous treatment that can induce CRM non-involvement (CRM-) should be considered even in early stages of rectal cancer.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
