Hantai Kim, Jungho Ha, Ga Young Gu, Yun-Hoon Choung
{"title":"中耳手术后骨传导听力改善机制的探讨。","authors":"Hantai Kim, Jungho Ha, Ga Young Gu, Yun-Hoon Choung","doi":"10.21053/ceo.2022.01039","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>When performing middle ear operations, such as ossiculoplasty or stapes surgery, patients and surgeons expect an improvement in air conduction (AC) hearing, but generally not in bone conduction (BC). However, BC improvement has often been observed after surgery, and the present study investigated this phenomenon.</p><p><strong>Methods: </strong>We reviewed the preoperative and postoperative surgical outcomes of 583 patients who underwent middle ear surgery. BC improvement was defined as a BC threshold decrease of >15 dB at two or more frequencies. Subjects in group A underwent staged ossiculoplasty after canal wall up mastoidectomy (CWUM), group B underwent staged ossiculoplasty after canal wall down mastoidectomy (CWDM), group C underwent ossiculoplasty only (thus, they had no prior history of CWUM or CWDM), and group D received stapes surgery. We created a hypothetical circuit model to explain this phenomenon.</p><p><strong>Results: </strong>BC improvement was detected in 12.8% of group A, 9.1% of group B, and 8.5% of group C. The improvement was more pronounced in group D (27.0%). A larger gain in AC hearing was weakly correlated with greater BC improvement (Pearson's r=0.395 in group A, P<0.001; r=0.375 in group B, P<0.001; r=0.296 in group C, P<0.001; r=0.422 in group D, P=0.009). Notably, patients with otosclerosis even experienced postoperative BC improvements as large as 10.0 dB, from a mean value of 30.3 dB (standard error [SE], 3.2) preoperatively to 20.3 dB (SE, 3.2) postoperatively, at 1,000 Hz, as well as an improvement of 9.2 dB at 2,000 Hz, from 37.8 dB (SE, 2.6) to 28.6 dB (SE, 3.1).</p><p><strong>Conclusion: </strong>BC improvement may be explained by a hypothetical circuit model applying the third window theory. Surgeons should keep in mind the possibility of BC improvement when making a management plan.</p>","PeriodicalId":10318,"journal":{"name":"Clinical and Experimental Otorhinolaryngology","volume":"16 1","pages":"20-27"},"PeriodicalIF":3.4000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e0/55/ceo-2022-01039.PMC9985987.pdf","citationCount":"0","resultStr":"{\"title\":\"Improved Bone Conduction Hearing After Middle Ear Surgery: Investigation of the Improvement Mechanism.\",\"authors\":\"Hantai Kim, Jungho Ha, Ga Young Gu, Yun-Hoon Choung\",\"doi\":\"10.21053/ceo.2022.01039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>When performing middle ear operations, such as ossiculoplasty or stapes surgery, patients and surgeons expect an improvement in air conduction (AC) hearing, but generally not in bone conduction (BC). However, BC improvement has often been observed after surgery, and the present study investigated this phenomenon.</p><p><strong>Methods: </strong>We reviewed the preoperative and postoperative surgical outcomes of 583 patients who underwent middle ear surgery. BC improvement was defined as a BC threshold decrease of >15 dB at two or more frequencies. Subjects in group A underwent staged ossiculoplasty after canal wall up mastoidectomy (CWUM), group B underwent staged ossiculoplasty after canal wall down mastoidectomy (CWDM), group C underwent ossiculoplasty only (thus, they had no prior history of CWUM or CWDM), and group D received stapes surgery. We created a hypothetical circuit model to explain this phenomenon.</p><p><strong>Results: </strong>BC improvement was detected in 12.8% of group A, 9.1% of group B, and 8.5% of group C. The improvement was more pronounced in group D (27.0%). A larger gain in AC hearing was weakly correlated with greater BC improvement (Pearson's r=0.395 in group A, P<0.001; r=0.375 in group B, P<0.001; r=0.296 in group C, P<0.001; r=0.422 in group D, P=0.009). Notably, patients with otosclerosis even experienced postoperative BC improvements as large as 10.0 dB, from a mean value of 30.3 dB (standard error [SE], 3.2) preoperatively to 20.3 dB (SE, 3.2) postoperatively, at 1,000 Hz, as well as an improvement of 9.2 dB at 2,000 Hz, from 37.8 dB (SE, 2.6) to 28.6 dB (SE, 3.1).</p><p><strong>Conclusion: </strong>BC improvement may be explained by a hypothetical circuit model applying the third window theory. Surgeons should keep in mind the possibility of BC improvement when making a management plan.</p>\",\"PeriodicalId\":10318,\"journal\":{\"name\":\"Clinical and Experimental Otorhinolaryngology\",\"volume\":\"16 1\",\"pages\":\"20-27\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e0/55/ceo-2022-01039.PMC9985987.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Otorhinolaryngology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21053/ceo.2022.01039\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Otorhinolaryngology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21053/ceo.2022.01039","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
Improved Bone Conduction Hearing After Middle Ear Surgery: Investigation of the Improvement Mechanism.
Objectives: When performing middle ear operations, such as ossiculoplasty or stapes surgery, patients and surgeons expect an improvement in air conduction (AC) hearing, but generally not in bone conduction (BC). However, BC improvement has often been observed after surgery, and the present study investigated this phenomenon.
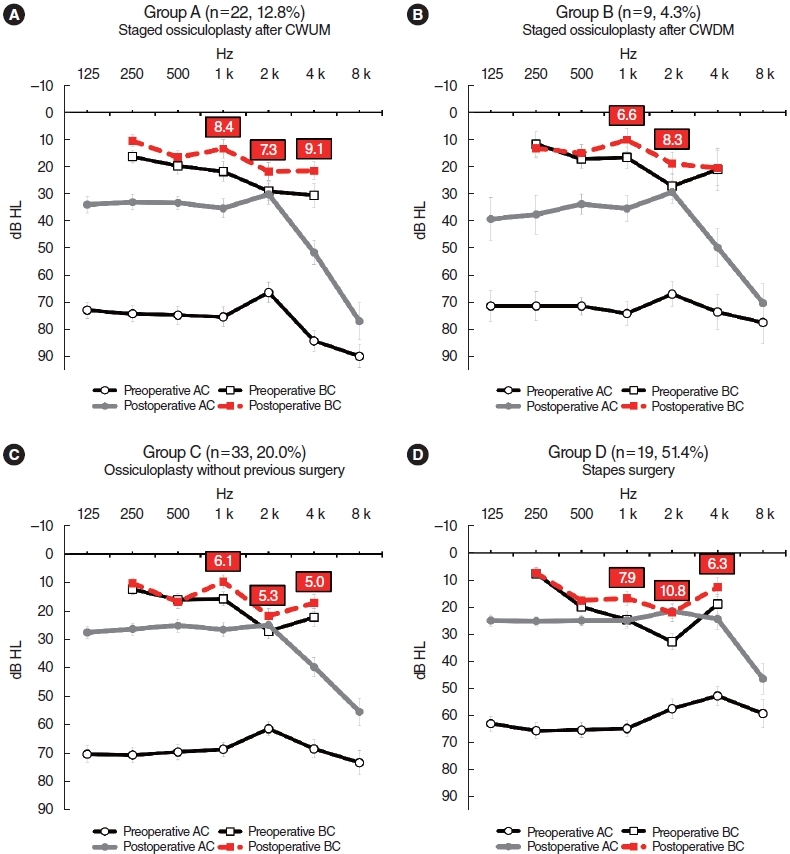
Methods: We reviewed the preoperative and postoperative surgical outcomes of 583 patients who underwent middle ear surgery. BC improvement was defined as a BC threshold decrease of >15 dB at two or more frequencies. Subjects in group A underwent staged ossiculoplasty after canal wall up mastoidectomy (CWUM), group B underwent staged ossiculoplasty after canal wall down mastoidectomy (CWDM), group C underwent ossiculoplasty only (thus, they had no prior history of CWUM or CWDM), and group D received stapes surgery. We created a hypothetical circuit model to explain this phenomenon.
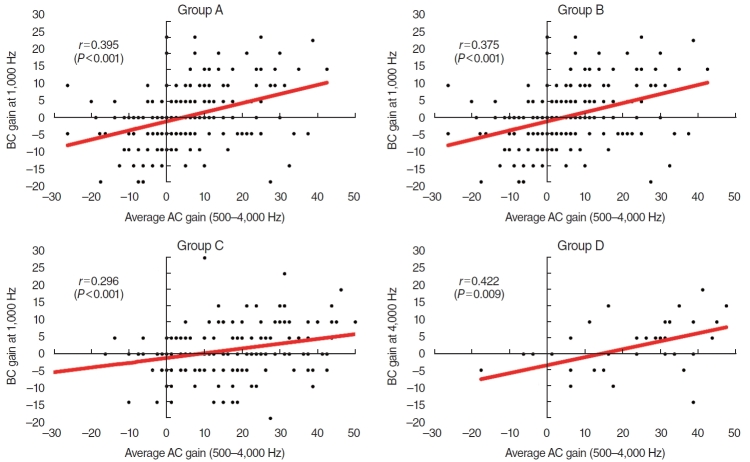
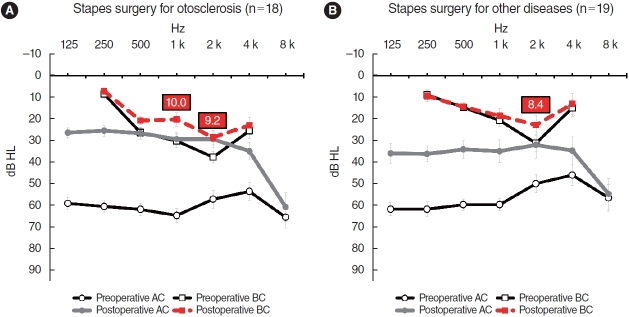
Results: BC improvement was detected in 12.8% of group A, 9.1% of group B, and 8.5% of group C. The improvement was more pronounced in group D (27.0%). A larger gain in AC hearing was weakly correlated with greater BC improvement (Pearson's r=0.395 in group A, P<0.001; r=0.375 in group B, P<0.001; r=0.296 in group C, P<0.001; r=0.422 in group D, P=0.009). Notably, patients with otosclerosis even experienced postoperative BC improvements as large as 10.0 dB, from a mean value of 30.3 dB (standard error [SE], 3.2) preoperatively to 20.3 dB (SE, 3.2) postoperatively, at 1,000 Hz, as well as an improvement of 9.2 dB at 2,000 Hz, from 37.8 dB (SE, 2.6) to 28.6 dB (SE, 3.1).
Conclusion: BC improvement may be explained by a hypothetical circuit model applying the third window theory. Surgeons should keep in mind the possibility of BC improvement when making a management plan.
期刊介绍:
Clinical and Experimental Otorhinolaryngology (Clin Exp Otorhinolaryngol, CEO) is an international peer-reviewed journal on recent developments in diagnosis and treatment of otorhinolaryngology-head and neck surgery and dedicated to the advancement of patient care in ear, nose, throat, head, and neck disorders. This journal publishes original articles relating to both clinical and basic researches, reviews, and clinical trials, encompassing the whole topics of otorhinolaryngology-head and neck surgery.
CEO was first issued in 2008 and this journal is published in English four times (the last day of February, May, August, and November) per year by the Korean Society of Otorhinolaryngology-Head and Neck Surgery. The Journal aims at publishing evidence-based, scientifically written articles from different disciplines of otorhinolaryngology field.
The readership contains clinical/basic research into current practice in otorhinolaryngology, audiology, speech pathology, head and neck oncology, plastic and reconstructive surgery. The readers are otolaryngologists, head and neck surgeons and oncologists, audiologists, and speech pathologists.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
