{"title":"杜氏肌营养不良症(DMD)的血管疗法。","authors":"Sangharsha Thapa, Shaymaa Elhadidy, Atsushi Asakura","doi":"10.12703/r/12-3","DOIUrl":null,"url":null,"abstract":"<p><p>Duchenne muscular dystrophy (DMD) is a progressive disease characterized by the wasting of the muscles that eventually lead to difficulty moving and, ultimately, premature death from heart and respiratory complications. DMD deficiency is caused by mutations in the gene encoding <i>dystrophin</i>, which prevents skeletal muscle, cardiac muscle, and other cells from producing the functional protein. Located on the cytoplasmic face of the plasma membrane of muscle fibers, dystrophin serves as a component of the dystrophin glycoprotein complex (DGC), mechanically reinforces the sarcolemma, and stabilizes the DGC, preventing it from contraction-mediated muscle degradation. In DMD muscle, <i>dystrophin</i> deficiency leads to progressive fibrosis, myofiber damage, chronic inflammation, and dysfunction of the mitochondria and muscle stem cells. Currently, DMD is incurable, and treatment involves the administration of glucocorticoids in order to delay disease progression. In the presence of developmental delay, proximal weakness, and elevated serum creatine kinase levels, a definitive diagnosis can usually be made after an extensive review of the patient's history and physical examination, as well as confirmation through muscle biopsy or genetic testing. Current standards of care include the use of corticosteroids to prolong ambulation and delay the onset of secondary complications, including respiratory muscle and cardiac functions. However, different studies have been carried out to show the relationship between vascular density and impaired angiogenesis in the pathogenesis of DMD. Several recent studies on DMD management are vascular targeted and focused on ischemia as a culprit for the pathogenesis of DMD. This review critically discusses approaches-such as modulation of nitric oxide (NO) or vascular endothelial growth factor (VEGF)-related pathways-to attenuate the dystrophic phenotype and enhance angiogenesis.</p>","PeriodicalId":73016,"journal":{"name":"Faculty reviews","volume":"12 ","pages":"3"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9979239/pdf/","citationCount":"0","resultStr":"{\"title\":\"Vascular therapy for Duchenne muscular dystrophy (DMD).\",\"authors\":\"Sangharsha Thapa, Shaymaa Elhadidy, Atsushi Asakura\",\"doi\":\"10.12703/r/12-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Duchenne muscular dystrophy (DMD) is a progressive disease characterized by the wasting of the muscles that eventually lead to difficulty moving and, ultimately, premature death from heart and respiratory complications. DMD deficiency is caused by mutations in the gene encoding <i>dystrophin</i>, which prevents skeletal muscle, cardiac muscle, and other cells from producing the functional protein. Located on the cytoplasmic face of the plasma membrane of muscle fibers, dystrophin serves as a component of the dystrophin glycoprotein complex (DGC), mechanically reinforces the sarcolemma, and stabilizes the DGC, preventing it from contraction-mediated muscle degradation. In DMD muscle, <i>dystrophin</i> deficiency leads to progressive fibrosis, myofiber damage, chronic inflammation, and dysfunction of the mitochondria and muscle stem cells. Currently, DMD is incurable, and treatment involves the administration of glucocorticoids in order to delay disease progression. In the presence of developmental delay, proximal weakness, and elevated serum creatine kinase levels, a definitive diagnosis can usually be made after an extensive review of the patient's history and physical examination, as well as confirmation through muscle biopsy or genetic testing. Current standards of care include the use of corticosteroids to prolong ambulation and delay the onset of secondary complications, including respiratory muscle and cardiac functions. However, different studies have been carried out to show the relationship between vascular density and impaired angiogenesis in the pathogenesis of DMD. Several recent studies on DMD management are vascular targeted and focused on ischemia as a culprit for the pathogenesis of DMD. This review critically discusses approaches-such as modulation of nitric oxide (NO) or vascular endothelial growth factor (VEGF)-related pathways-to attenuate the dystrophic phenotype and enhance angiogenesis.</p>\",\"PeriodicalId\":73016,\"journal\":{\"name\":\"Faculty reviews\",\"volume\":\"12 \",\"pages\":\"3\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9979239/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Faculty reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12703/r/12-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Faculty reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12703/r/12-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Vascular therapy for Duchenne muscular dystrophy (DMD).
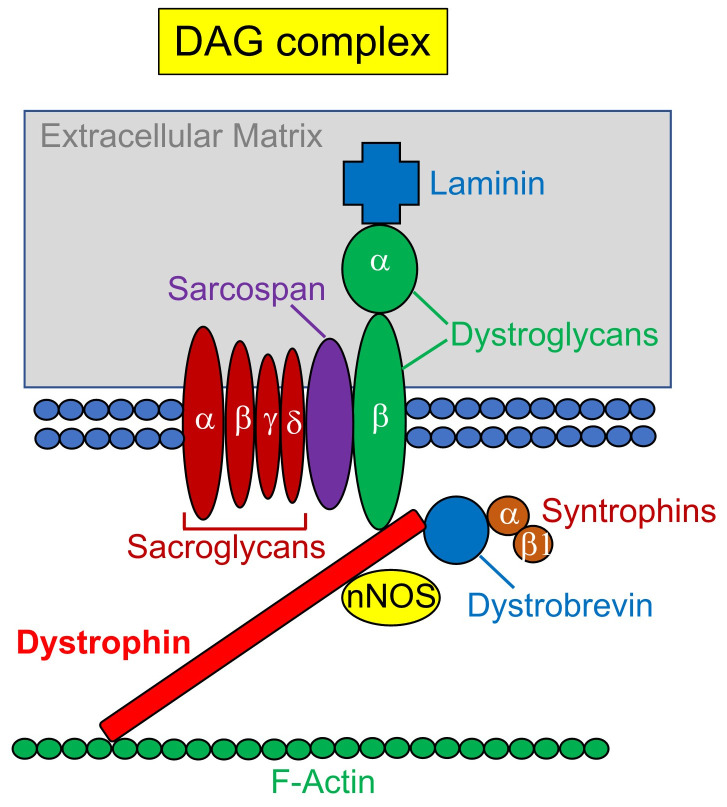
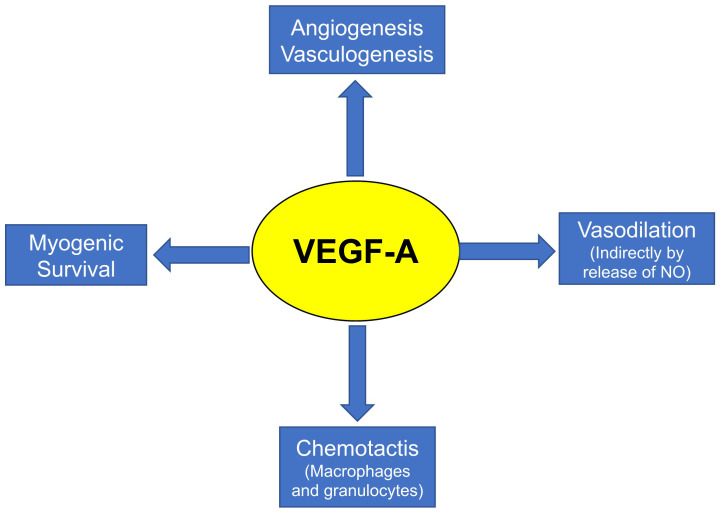
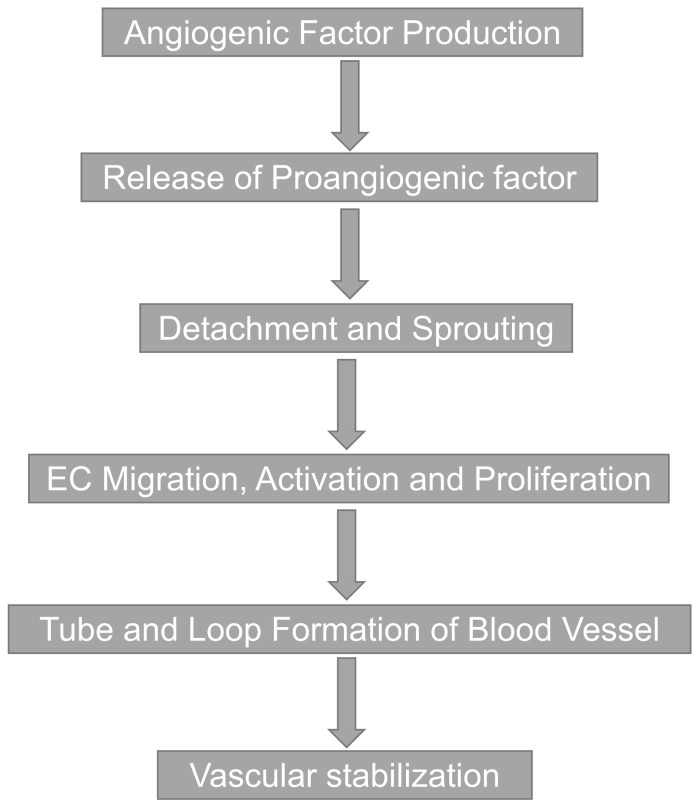
Duchenne muscular dystrophy (DMD) is a progressive disease characterized by the wasting of the muscles that eventually lead to difficulty moving and, ultimately, premature death from heart and respiratory complications. DMD deficiency is caused by mutations in the gene encoding dystrophin, which prevents skeletal muscle, cardiac muscle, and other cells from producing the functional protein. Located on the cytoplasmic face of the plasma membrane of muscle fibers, dystrophin serves as a component of the dystrophin glycoprotein complex (DGC), mechanically reinforces the sarcolemma, and stabilizes the DGC, preventing it from contraction-mediated muscle degradation. In DMD muscle, dystrophin deficiency leads to progressive fibrosis, myofiber damage, chronic inflammation, and dysfunction of the mitochondria and muscle stem cells. Currently, DMD is incurable, and treatment involves the administration of glucocorticoids in order to delay disease progression. In the presence of developmental delay, proximal weakness, and elevated serum creatine kinase levels, a definitive diagnosis can usually be made after an extensive review of the patient's history and physical examination, as well as confirmation through muscle biopsy or genetic testing. Current standards of care include the use of corticosteroids to prolong ambulation and delay the onset of secondary complications, including respiratory muscle and cardiac functions. However, different studies have been carried out to show the relationship between vascular density and impaired angiogenesis in the pathogenesis of DMD. Several recent studies on DMD management are vascular targeted and focused on ischemia as a culprit for the pathogenesis of DMD. This review critically discusses approaches-such as modulation of nitric oxide (NO) or vascular endothelial growth factor (VEGF)-related pathways-to attenuate the dystrophic phenotype and enhance angiogenesis.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
