Talayeh S Ghezelayagh, Emily S Wu, Emma L Barber, Minh D Dao, Emese Zsiros, Renata R Urban, Heidi J Gray, Barbara A Goff, Chirag A Shah, Nikki L Neubauer, James Y Dai, Janos L Tanyi, John B Liao
{"title":"贝伐单抗治疗的时间和持续时间以及复发性卵巢癌、输卵管癌和腹膜癌患者的生存:一项多机构研究","authors":"Talayeh S Ghezelayagh, Emily S Wu, Emma L Barber, Minh D Dao, Emese Zsiros, Renata R Urban, Heidi J Gray, Barbara A Goff, Chirag A Shah, Nikki L Neubauer, James Y Dai, Janos L Tanyi, John B Liao","doi":"10.22514/ejgo.2023.002","DOIUrl":null,"url":null,"abstract":"<p><p>Bevacizumab has demonstrated significant benefit in recurrent ovarian, fallopian tube and peritoneal cancer (OC), but its optimal position within the sequence of systemic therapies remains controversial. Since rebound progression after bevacizumab has been observed in other cancers, and because bevacizumab is incorporated in several regimens used in the recurrent setting, the duration of treatment may impact survival. We sought to identify whether earlier bevacizumab exposure is associated with prolonged bevacizumab therapy and survival by conducting a multi-institution retrospective study of recurrent OC patients treated with bevacizumab from 2004-2014. Multivariate logistic regression identified factors associated with receiving more than six bevacizumab cycles. Overall survival by duration and ordinal sequence of bevacizumab therapy were evaluated using logrank testing and Cox regression. In total, 318 patients were identified. 89.1% had stage III or IV disease; 36% had primary platinum resistance; 40.5% received two or fewer prior chemotherapy regimens. Multivariate logistic regression demonstrated that primary platinum sensitivity (Odds Ratio (OR) 2.34, <i>p</i> = 0.001) or initiating bevacizumab at the first or second recurrence (OR 2.73, <i>p</i> < 0.001) were independently associated with receiving more than six cycles of bevacizumab. Receiving more cycles of bevacizumab was associated with improved overall survival whether measured from time of diagnosis (logrank <i>p</i> < 0.001), bevacizumab initiation (logrank <i>p</i> < 0.001), or bevacizumab discontinuation (logrank <i>p</i> = 0.017). Waiting one additional recurrence to initiate bevacizumab resulted in a 27% increased hazard of death (Hazard Ratio (HR) 1.27, <i>p</i> < 0.001) by multivariate analysis. In conclusion, patients with primary platinum sensitive disease who received fewer prior lines of chemotherapy were able to receive more cycles of bevacizumab, which was associated with improved overall survival. Survival worsened when bevacizumab was initiated later in the ordinal sequence of therapies.</p>","PeriodicalId":11903,"journal":{"name":"European journal of gynaecological oncology","volume":"44 1","pages":"17-25"},"PeriodicalIF":0.5000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9980410/pdf/","citationCount":"1","resultStr":"{\"title\":\"Timing and duration of bevacizumab treatment and survival in patients with recurrent ovarian, fallopian tube, and peritoneal cancer: a multi-institution study.\",\"authors\":\"Talayeh S Ghezelayagh, Emily S Wu, Emma L Barber, Minh D Dao, Emese Zsiros, Renata R Urban, Heidi J Gray, Barbara A Goff, Chirag A Shah, Nikki L Neubauer, James Y Dai, Janos L Tanyi, John B Liao\",\"doi\":\"10.22514/ejgo.2023.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Bevacizumab has demonstrated significant benefit in recurrent ovarian, fallopian tube and peritoneal cancer (OC), but its optimal position within the sequence of systemic therapies remains controversial. Since rebound progression after bevacizumab has been observed in other cancers, and because bevacizumab is incorporated in several regimens used in the recurrent setting, the duration of treatment may impact survival. We sought to identify whether earlier bevacizumab exposure is associated with prolonged bevacizumab therapy and survival by conducting a multi-institution retrospective study of recurrent OC patients treated with bevacizumab from 2004-2014. Multivariate logistic regression identified factors associated with receiving more than six bevacizumab cycles. Overall survival by duration and ordinal sequence of bevacizumab therapy were evaluated using logrank testing and Cox regression. In total, 318 patients were identified. 89.1% had stage III or IV disease; 36% had primary platinum resistance; 40.5% received two or fewer prior chemotherapy regimens. Multivariate logistic regression demonstrated that primary platinum sensitivity (Odds Ratio (OR) 2.34, <i>p</i> = 0.001) or initiating bevacizumab at the first or second recurrence (OR 2.73, <i>p</i> < 0.001) were independently associated with receiving more than six cycles of bevacizumab. Receiving more cycles of bevacizumab was associated with improved overall survival whether measured from time of diagnosis (logrank <i>p</i> < 0.001), bevacizumab initiation (logrank <i>p</i> < 0.001), or bevacizumab discontinuation (logrank <i>p</i> = 0.017). Waiting one additional recurrence to initiate bevacizumab resulted in a 27% increased hazard of death (Hazard Ratio (HR) 1.27, <i>p</i> < 0.001) by multivariate analysis. In conclusion, patients with primary platinum sensitive disease who received fewer prior lines of chemotherapy were able to receive more cycles of bevacizumab, which was associated with improved overall survival. Survival worsened when bevacizumab was initiated later in the ordinal sequence of therapies.</p>\",\"PeriodicalId\":11903,\"journal\":{\"name\":\"European journal of gynaecological oncology\",\"volume\":\"44 1\",\"pages\":\"17-25\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9980410/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of gynaecological oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.22514/ejgo.2023.002\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of gynaecological oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.22514/ejgo.2023.002","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
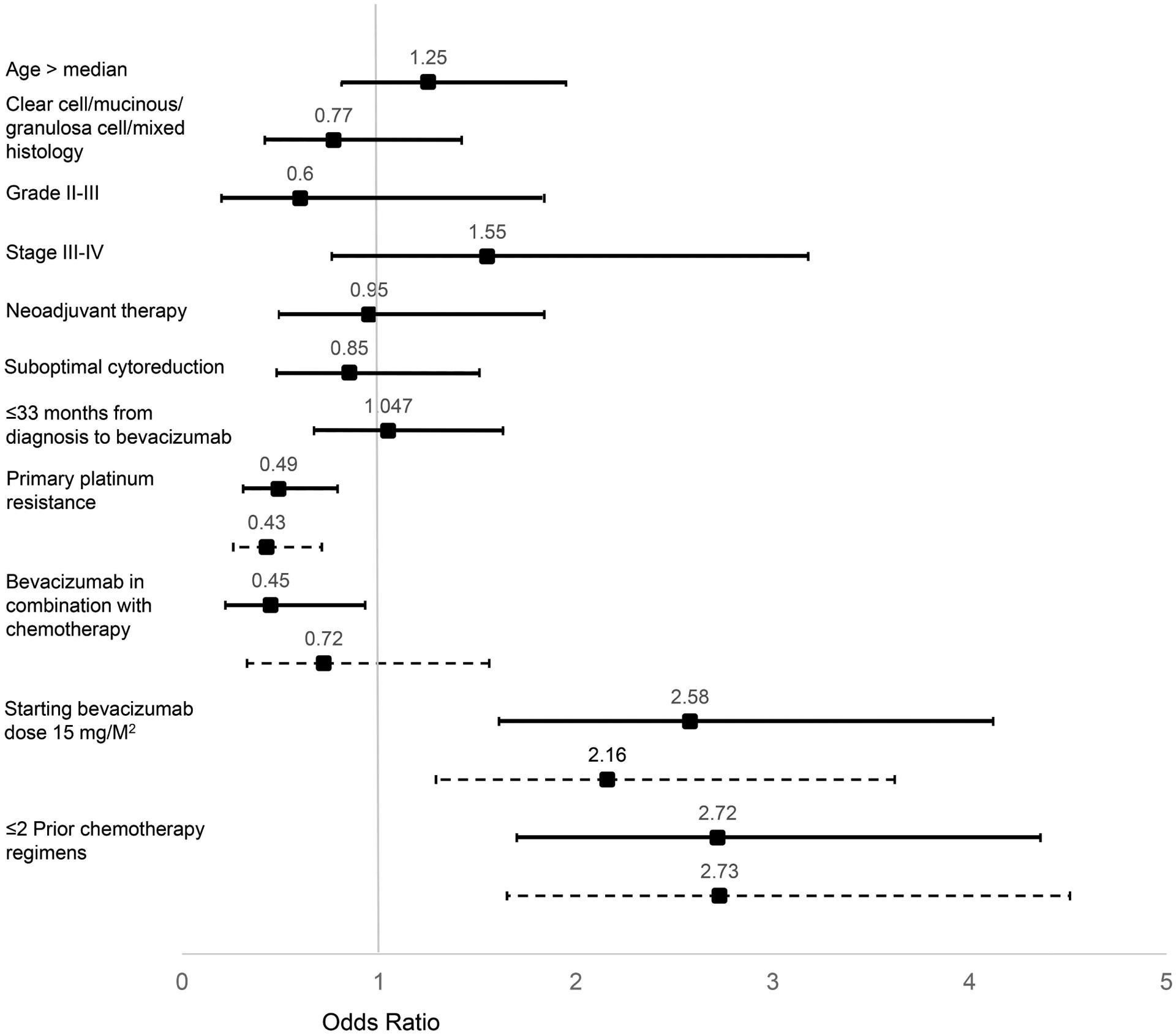
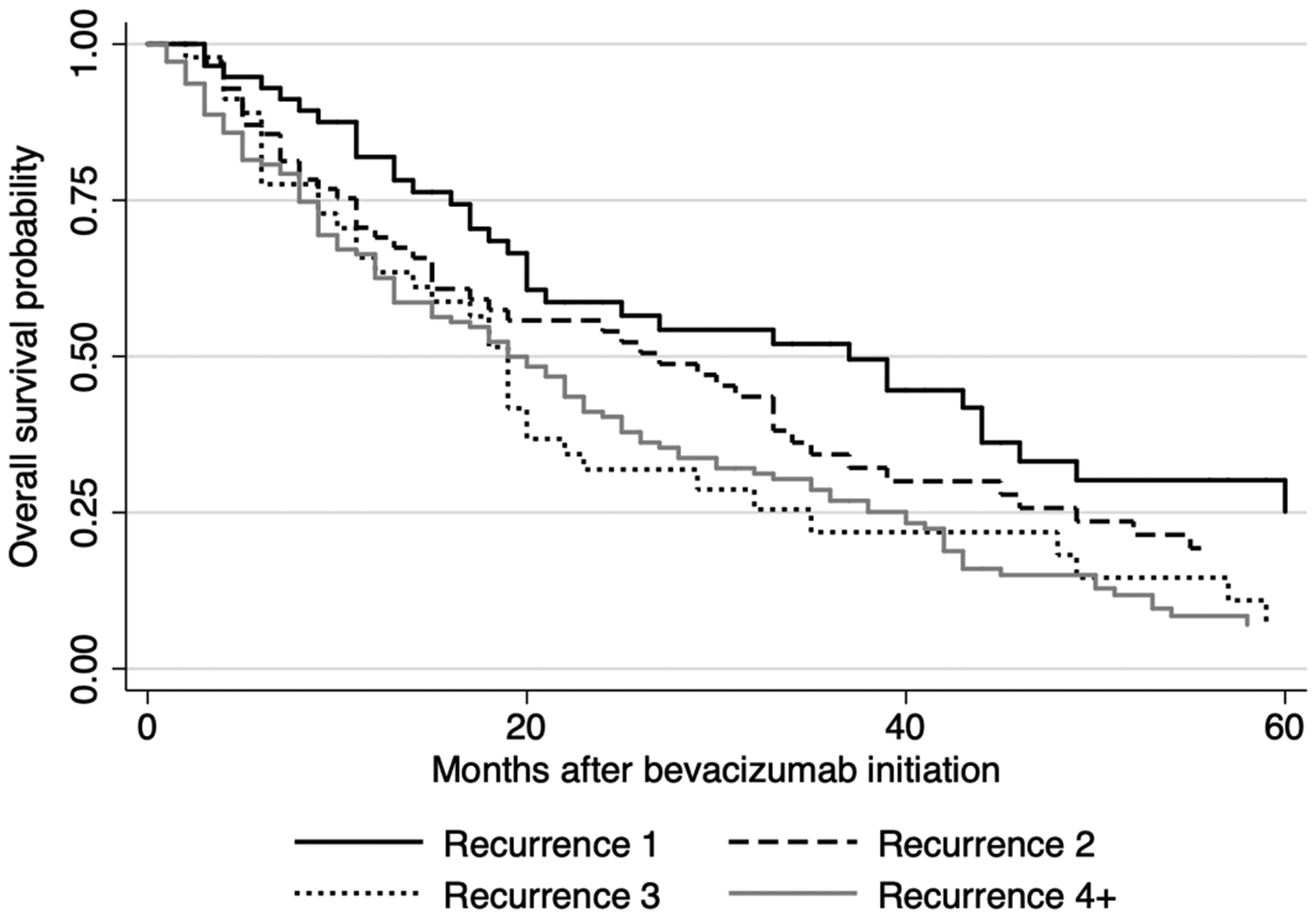
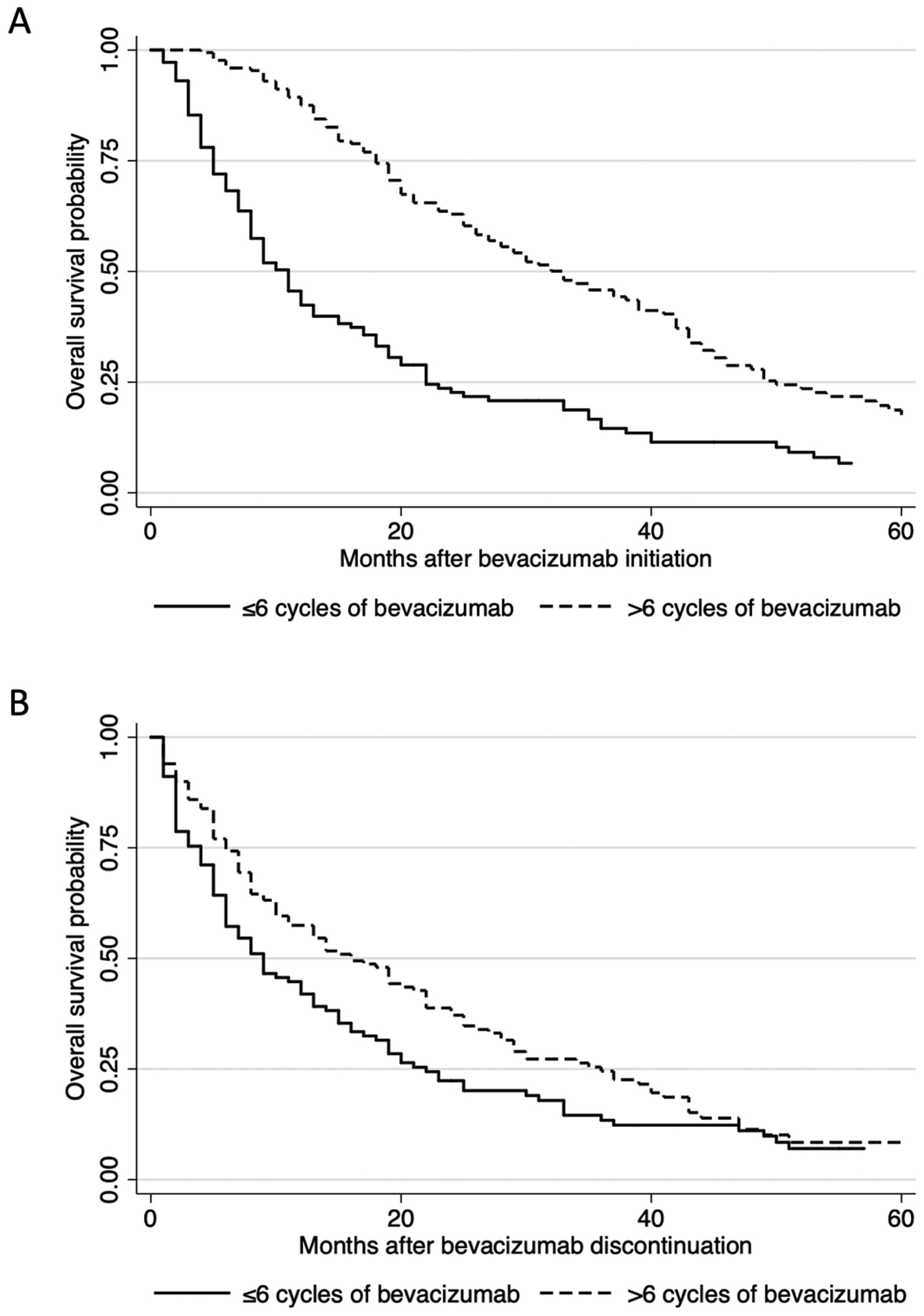
贝伐单抗在复发性卵巢癌、输卵管癌和腹膜癌(OC)中显示出显著的益处,但其在全身治疗序列中的最佳位置仍存在争议。由于在其他癌症中观察到贝伐珠单抗后的反弹进展,并且由于贝伐珠单抗被合并在复发环境中使用的几种方案中,治疗的持续时间可能影响生存。我们通过对2004-2014年接受贝伐单抗治疗的复发性OC患者进行多机构回顾性研究,试图确定早期贝伐单抗暴露是否与延长贝伐单抗治疗和生存率相关。多变量logistic回归确定了接受6个以上贝伐单抗周期的相关因素。使用洛格兰试验和Cox回归评估贝伐单抗治疗持续时间和顺序序列的总生存期。总共确定了318例患者。89.1%为III期或IV期;36%有初级铂电阻;40.5%接受过两次或更少的化疗方案。多因素logistic回归显示,原发性铂敏感性(比值比(OR) 2.34, p = 0.001)或在第一次或第二次复发时开始使用贝伐单抗(OR 2.73, p < 0.001)与接受贝伐单抗治疗超过6个周期独立相关。无论从诊断时间(洛格兰p < 0.001)、贝伐珠单抗起始(洛格兰p < 0.001)还是贝伐珠单抗停药(洛格兰p = 0.017)开始测量,接受更多周期的贝伐珠单抗与改善的总生存率相关。多因素分析显示,等待一次复发再开始使用贝伐单抗导致死亡风险增加27%(风险比(HR) 1.27, p < 0.001)。总之,既往接受较少化疗的原发性铂敏感疾病患者能够接受更多周期的贝伐单抗治疗,这与改善的总生存期相关。当贝伐单抗在常规治疗序列中较晚开始时,生存率恶化。
Timing and duration of bevacizumab treatment and survival in patients with recurrent ovarian, fallopian tube, and peritoneal cancer: a multi-institution study.
Bevacizumab has demonstrated significant benefit in recurrent ovarian, fallopian tube and peritoneal cancer (OC), but its optimal position within the sequence of systemic therapies remains controversial. Since rebound progression after bevacizumab has been observed in other cancers, and because bevacizumab is incorporated in several regimens used in the recurrent setting, the duration of treatment may impact survival. We sought to identify whether earlier bevacizumab exposure is associated with prolonged bevacizumab therapy and survival by conducting a multi-institution retrospective study of recurrent OC patients treated with bevacizumab from 2004-2014. Multivariate logistic regression identified factors associated with receiving more than six bevacizumab cycles. Overall survival by duration and ordinal sequence of bevacizumab therapy were evaluated using logrank testing and Cox regression. In total, 318 patients were identified. 89.1% had stage III or IV disease; 36% had primary platinum resistance; 40.5% received two or fewer prior chemotherapy regimens. Multivariate logistic regression demonstrated that primary platinum sensitivity (Odds Ratio (OR) 2.34, p = 0.001) or initiating bevacizumab at the first or second recurrence (OR 2.73, p < 0.001) were independently associated with receiving more than six cycles of bevacizumab. Receiving more cycles of bevacizumab was associated with improved overall survival whether measured from time of diagnosis (logrank p < 0.001), bevacizumab initiation (logrank p < 0.001), or bevacizumab discontinuation (logrank p = 0.017). Waiting one additional recurrence to initiate bevacizumab resulted in a 27% increased hazard of death (Hazard Ratio (HR) 1.27, p < 0.001) by multivariate analysis. In conclusion, patients with primary platinum sensitive disease who received fewer prior lines of chemotherapy were able to receive more cycles of bevacizumab, which was associated with improved overall survival. Survival worsened when bevacizumab was initiated later in the ordinal sequence of therapies.
期刊介绍:
EJGO is dedicated to publishing editorial articles in the Distinguished Expert Series and original research papers, case reports, letters to the Editor, book reviews, and newsletters. The Journal was founded in 1980 the second gynaecologic oncology hyperspecialization Journal in the world. Its aim is the diffusion of scientific, clinical and practical progress, and knowledge in female neoplastic diseases in an interdisciplinary approach among gynaecologists, oncologists, radiotherapists, surgeons, chemotherapists, pathologists, epidemiologists, and so on.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
