Colleen L. MacCallum-Bridges PhD, MS, Jana L. Hirschtick PhD, MPH, Kristi L. Allgood PhD, MPH, Soomin Ryu PhD, MA, Robert C. Orellana PhD, MPH, Nancy L. Fleischer PhD, MPH
{"title":"2020-2022年密歇根聚合酶链反应确诊COVID-19成人长冠状病毒流行率城乡差异的横断面人口估计","authors":"Colleen L. MacCallum-Bridges PhD, MS, Jana L. Hirschtick PhD, MPH, Kristi L. Allgood PhD, MPH, Soomin Ryu PhD, MA, Robert C. Orellana PhD, MPH, Nancy L. Fleischer PhD, MPH","doi":"10.1111/jrh.12807","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Purpose</h3>\n \n <p>To (1) assess whether residential rurality/urbanicity was associated with the prevalence of 30- or 90-day long COVID, and (2) evaluate whether differences in long COVID risk factors might explain this potential disparity.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We used data from the Michigan COVID-19 Recovery Surveillance Study, a population-based probability sample of adults with COVID-19 (n = 4,937). We measured residential rurality/urbanicity using dichotomized Rural-Urban Commuting Area codes (metropolitan, nonmetropolitan). We considered outcomes of 30-day long COVID (illness duration ≥30 days) and 90-day long COVID (illness duration ≥90 days). Using Poisson regression, we estimated unadjusted prevalence ratios (PRs) to compare 30- and 90-day long COVID between metropolitan and nonmetropolitan respondents. Then, we adjusted our model to account for differences between groups in long COVID risk factors (age, sex, acute COVID-19 severity, vaccination status, race and ethnicity, socioeconomic status, health care access, SARS-CoV-2 variant, and pre-existing conditions). We estimated associations for the full study period (Jan 1, 2020-May 31, 2022), the pre-vaccine era (before April 5, 2021), and the vaccine era (after April 5, 2021).</p>\n </section>\n \n <section>\n \n <h3> Findings</h3>\n \n <p>Compared to metropolitan adults, the prevalence of 30-day long COVID was 15% higher (PR = 1.15 [95% CI: 1.03, 1.29]), and the prevalence of 90-day long COVID was 27% higher (PR = 1.27 [95% CI: 1.09, 1.49]) among nonmetropolitan adults. Adjusting for long COVID risk factors did not reduce disparity estimates in the pre-vaccine era but halved estimates in the vaccine era.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our findings provide evidence of a rural-urban disparity in long COVID and suggest that the factors contributing to this disparity changed over time as the sociopolitical context of the pandemic evolved and COVID-19 vaccines were introduced.</p>\n </section>\n </div>","PeriodicalId":50060,"journal":{"name":"Journal of Rural Health","volume":"40 2","pages":"303-313"},"PeriodicalIF":2.7000,"publicationDate":"2023-11-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jrh.12807","citationCount":"0","resultStr":"{\"title\":\"Cross-sectional population-based estimates of a rural-urban disparity in prevalence of long COVID among Michigan adults with polymerase chain reaction-confirmed COVID-19, 2020-2022\",\"authors\":\"Colleen L. MacCallum-Bridges PhD, MS, Jana L. Hirschtick PhD, MPH, Kristi L. Allgood PhD, MPH, Soomin Ryu PhD, MA, Robert C. Orellana PhD, MPH, Nancy L. Fleischer PhD, MPH\",\"doi\":\"10.1111/jrh.12807\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Purpose</h3>\\n \\n <p>To (1) assess whether residential rurality/urbanicity was associated with the prevalence of 30- or 90-day long COVID, and (2) evaluate whether differences in long COVID risk factors might explain this potential disparity.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We used data from the Michigan COVID-19 Recovery Surveillance Study, a population-based probability sample of adults with COVID-19 (n = 4,937). We measured residential rurality/urbanicity using dichotomized Rural-Urban Commuting Area codes (metropolitan, nonmetropolitan). We considered outcomes of 30-day long COVID (illness duration ≥30 days) and 90-day long COVID (illness duration ≥90 days). Using Poisson regression, we estimated unadjusted prevalence ratios (PRs) to compare 30- and 90-day long COVID between metropolitan and nonmetropolitan respondents. Then, we adjusted our model to account for differences between groups in long COVID risk factors (age, sex, acute COVID-19 severity, vaccination status, race and ethnicity, socioeconomic status, health care access, SARS-CoV-2 variant, and pre-existing conditions). We estimated associations for the full study period (Jan 1, 2020-May 31, 2022), the pre-vaccine era (before April 5, 2021), and the vaccine era (after April 5, 2021).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Findings</h3>\\n \\n <p>Compared to metropolitan adults, the prevalence of 30-day long COVID was 15% higher (PR = 1.15 [95% CI: 1.03, 1.29]), and the prevalence of 90-day long COVID was 27% higher (PR = 1.27 [95% CI: 1.09, 1.49]) among nonmetropolitan adults. Adjusting for long COVID risk factors did not reduce disparity estimates in the pre-vaccine era but halved estimates in the vaccine era.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Our findings provide evidence of a rural-urban disparity in long COVID and suggest that the factors contributing to this disparity changed over time as the sociopolitical context of the pandemic evolved and COVID-19 vaccines were introduced.</p>\\n </section>\\n </div>\",\"PeriodicalId\":50060,\"journal\":{\"name\":\"Journal of Rural Health\",\"volume\":\"40 2\",\"pages\":\"303-313\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2023-11-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jrh.12807\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Rural Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jrh.12807\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Rural Health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jrh.12807","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Cross-sectional population-based estimates of a rural-urban disparity in prevalence of long COVID among Michigan adults with polymerase chain reaction-confirmed COVID-19, 2020-2022
Purpose
To (1) assess whether residential rurality/urbanicity was associated with the prevalence of 30- or 90-day long COVID, and (2) evaluate whether differences in long COVID risk factors might explain this potential disparity.
Methods
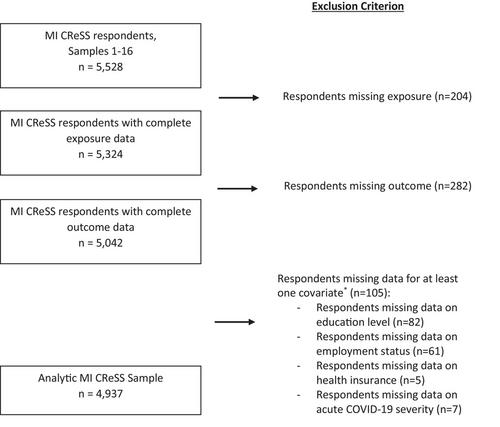
We used data from the Michigan COVID-19 Recovery Surveillance Study, a population-based probability sample of adults with COVID-19 (n = 4,937). We measured residential rurality/urbanicity using dichotomized Rural-Urban Commuting Area codes (metropolitan, nonmetropolitan). We considered outcomes of 30-day long COVID (illness duration ≥30 days) and 90-day long COVID (illness duration ≥90 days). Using Poisson regression, we estimated unadjusted prevalence ratios (PRs) to compare 30- and 90-day long COVID between metropolitan and nonmetropolitan respondents. Then, we adjusted our model to account for differences between groups in long COVID risk factors (age, sex, acute COVID-19 severity, vaccination status, race and ethnicity, socioeconomic status, health care access, SARS-CoV-2 variant, and pre-existing conditions). We estimated associations for the full study period (Jan 1, 2020-May 31, 2022), the pre-vaccine era (before April 5, 2021), and the vaccine era (after April 5, 2021).
Findings
Compared to metropolitan adults, the prevalence of 30-day long COVID was 15% higher (PR = 1.15 [95% CI: 1.03, 1.29]), and the prevalence of 90-day long COVID was 27% higher (PR = 1.27 [95% CI: 1.09, 1.49]) among nonmetropolitan adults. Adjusting for long COVID risk factors did not reduce disparity estimates in the pre-vaccine era but halved estimates in the vaccine era.
Conclusions
Our findings provide evidence of a rural-urban disparity in long COVID and suggest that the factors contributing to this disparity changed over time as the sociopolitical context of the pandemic evolved and COVID-19 vaccines were introduced.
期刊介绍:
The Journal of Rural Health, a quarterly journal published by the NRHA, offers a variety of original research relevant and important to rural health. Some examples include evaluations, case studies, and analyses related to health status and behavior, as well as to health work force, policy and access issues. Quantitative, qualitative and mixed methods studies are welcome. Highest priority is given to manuscripts that reflect scholarly quality, demonstrate methodological rigor, and emphasize practical implications. The journal also publishes articles with an international rural health perspective, commentaries, book reviews and letters.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
