{"title":"脾切除术的重新评价:弥合免疫细胞减少治疗范式的差距。","authors":"Christina Waldron, George Goshua","doi":"10.1111/joim.13756","DOIUrl":null,"url":null,"abstract":"<p>The spleen is often the primary site of autoantibody production and autoantibody-coated clearance of hematologic cells in several immune-mediated hematologic rare diseases collectively referred to as autoimmune cytopenias. The affected hematologic cell lines in autoimmune cytopenia disorders most commonly include platelets, red cells, and neutrophils, with the respective conditions referred to as immune thrombocytopenic purpura (ITP), warm autoimmune hemolytic anemia (wAIHA), and autoimmune neutropenia (AIN). When two of these conditions co-occur, the immune-mediated hematologic process is referred to as Evans Syndrome (ES), named after Dr. Robert Evans who in 1951 first described the association of the former two diagnoses [<span>1</span>]. The eponym was then extended to include the possibility of AIN in the 1990s, a diagnosis with pathophysiology suggestive of the causal involvement of antineutrophil antibodies in 1975 [<span>2</span>].</p><p>The 2023 treatment considerations for AIN, when treatment is needed, include granulocyte-colony stimulating factor and/or immunosuppression, whereas the recommended first- and second-line treatment paradigms for ITP, wAIHA, and ES include immunosuppression anchored on corticosteroids and the monoclonal anti-CD20 rituximab, with additional consideration in the case of ITP for thrombopoietic agents referred to as thrombopoietin receptor agonists [<span>3-6</span>]. Third-line treatment includes additional immunosuppressant considerations, such as azathioprine and cyclosporine, and most recently, splenectomy, as a now-downgraded (i.e., third-line) therapeutic modality [<span>4-6</span>].</p><p>For ITP and wAIHA, and by extension their overlap known as ES, splenectomy was the preferred second-line treatment for over 50 years through the 2010s, being recommended by leading experts as recently as 2010 and 2011 for AIHA and ITP, respectively [<span>7, 8</span>]. As experience with the off-label use of rituximab grew, splenectomy increasingly drifted toward third-line treatment status due to concern of the tripartite risk of infection, thrombosis, and perioperative mortality [<span>4, 6</span>]. The point estimates for these risks, however, date to the 1990s and 2000s, and so predate advances in preoperative vaccination, thromboprophylaxis, and the laparoscopic approach to splenectomy. Nevertheless, and without the quantification of total splenectomy risk through the 2010s, splenectomy-associated risks have been qualitatively noted as likely too great. In our experience at the bedside, this has led to questions of appropriate patient counseling and informed consent. This is especially the case for individuals whose values and preferences align with pursuing a potentially one-time, definitive treatment, but who are dissuaded from pursuing splenectomy because the “risks are too great.” The issue does not exist on a population level, where we know that splenectomy continues to be the therapeutic modality with the highest probability of documented, long-term effectiveness without need for continuous therapy. Rather, the issue exists at the crucial individual level, where clinicians worry that we often cannot adequately adjust the pretest probability for the risk of disease recurrence after splenectomy for individual patients. Due to both ethical and practical considerations, we will never have prospective, randomized trial data to make these decisions. And yet these decisions need to be made, ideally with consent that is as informed as data limitations ultimately allow.</p><p>It is in this context of the absence of planned prospective data collection in this arena that, in this issue of the <i>Journal of Internal Medicine</i>, Ogbue et al. provide crucial insights of their institutional experience with splenectomy in the treatment of patients with a variety of autoimmune cytopenias at the Cleveland Clinic, an institution in the United States with a deep commitment to clinical excellence [<span>9</span>]. The authors meticulously applied thoughtful exclusion criteria through a retrospective evaluation of 1824 consecutive splenectomy cases across the years 2002–2020 to properly isolate 339 patients who underwent splenectomy for one of the following autoimmune cytopenia diagnoses with a subsequent median follow-up of 5 years: ITP (<i>n</i> = 235), AIHA (<i>n</i> = 68), ES (<i>n</i> = 26), and AIN (<i>n</i> = 10). Of particular importance, they report (1) appropriately adjudicated (i.e., disease-definition-specific) response and relapse rates at each yearly interval of follow-up for each autoimmune cytopenia; (2) complication rates accrued in per person-years for infection, thrombosis, and mortality; (3) patient vaccination status; (4) postoperative complications; and (5) pathology-proven discordant diagnoses appropriately removed from effectiveness metrics (Fig. 1). The authors additionally utilized their sample size to perform logistic regression across an appropriate maximum amount of risk factors to identify covariates that may be associated with favorable and unfavorable response to splenectomy.</p><p>Specifically, the authors report a robust 74% overall hematologic response rate with a 12% relapse rate; rates that have historically been expected with splenectomy across cohorts of individuals with the considered autoimmune cytopenias. Additionally, surgical complication rates and long-term morbidity were low, and this is despite a patient cohort that appears to be notably under-vaccinated for splenectomy, an issue that has been noted previously in modern medicine [<span>10</span>]. The authors attempted to identify key clinical covariates that are associated with both favorable and unfavorable responses to splenectomy. Although several were identified on univariable analyses, multivariable regression identified preoperative refractoriness or relapse after multiple lines of therapy as associated with splenectomy treatment failure. Arguably the most striking aspect of their study lies in their reporting of the value added of splenectomy as a diagnostic tool, in addition to its therapeutic potency. In 13% of all patients who underwent splenectomy, tissue diagnosis yielded a diagnosis that was discordant from the working diagnosis prior to splenectomy. The correct diagnoses largely included a variety of malignancies that have entirely different treatment paradigms, with most representing different types of lymphoma, which are notorious for difficulty of diagnosis when confined to the spleen and are known to drive immune-mediated hematologic findings that can resemble some autoimmune cytopenias.</p><p>Ogbue et al. are to be commended for conducting a rigorous retrospective analysis across heterogeneous conditions in a way that has added value to the field for patients and physicians. These findings buttress an increasing base of information within an important knowledge gap regarding splenectomy risks, the presence of which over the years has convinced some of our patients to stay away from splenectomy without properly informed consent. The authors also showcase the additional value of splenectomy for patients in making the correct diagnosis, even in the context of an institution known globally for clinical excellence. As important, properly reported rates in per-person-years of this well-annotated cohort provide a bevy of information that will be useful to researchers in health decision science and separately for researchers who may opt to pursue the creation of a patient decision aid in this space. Most important, it provides a well-done study beyond the ITP arena, with an additional focus on wAIHA and ES, that will incrementally help improve patient–physician shared decision-making in these treatment arenas.</p><p>As with all retrospective analyses, however, there are notable limitations. The work, in its nature, cannot be predictive. The sample sizes, although superb for rare disease work, are also relatively small, and the diseases under study are notably heterogeneous. Similar work at other institutions, particularly for diseases other than primary ITP, where there is substantially more data than in wAIHA and ES, would be helpful to confirm the effectiveness data. Most important, our patients are making a lifelong, unalterable decision when it comes to pursuing splenectomy, and so data well beyond a median follow-up of 5 years is needed. Thankfully, we now have data out to 20 years in ITP in at least one report, but similar data is lacking for wAIHA and ES. In addition, no generalizable conclusions should be drawn on the effectiveness of splenectomy for individuals with AIN given the very small sample size. Finally, the identified covariates associated with response, or lack thereof, to splenectomy are important confirmations and are not novel for practicing clinicians: The issue regarding uncertainty for patient selection for the splenectomy modality will continue.</p><p>Nevertheless, despite the limitations and even in the context of wonderful non-surgical therapeutic options, Ogbue et al. add sufficient data to remind us that splenectomy as a third-line option is inappropriate for all patients with autoimmune cytopenias. They additionally provide new data as to the risk of postsplenectomy infection while noting that the period under study does not exclusively span the modern vaccination era and that many patients may have been notably under-vaccinated. These are opportunities for the field and for our patients. As we continue to re-appraise the value of splenectomy, we need to ensure that all patients opting for the <i>possibility</i> of definitive, one-time treatment receive all recommended vaccinations and undergo appropriate discussion and risk stratification that considers their individual-specific covariates when it comes to thromboprophylaxis and the surgical approach. This would allow a true alignment of clinical care with patient values and preferences, in the context of known uncertainty and expected comparative data limitations when it comes to splenectomy consideration for all individuals living with autoimmune cytopenias.</p><p>The authors have no conflicts of interest to declare.</p>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"295 2","pages":"120-122"},"PeriodicalIF":9.2000,"publicationDate":"2023-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.13756","citationCount":"0","resultStr":"{\"title\":\"Splenectomy reappraised: Bridging the gap in immune cytopenia treatment paradigms\",\"authors\":\"Christina Waldron, George Goshua\",\"doi\":\"10.1111/joim.13756\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The spleen is often the primary site of autoantibody production and autoantibody-coated clearance of hematologic cells in several immune-mediated hematologic rare diseases collectively referred to as autoimmune cytopenias. The affected hematologic cell lines in autoimmune cytopenia disorders most commonly include platelets, red cells, and neutrophils, with the respective conditions referred to as immune thrombocytopenic purpura (ITP), warm autoimmune hemolytic anemia (wAIHA), and autoimmune neutropenia (AIN). When two of these conditions co-occur, the immune-mediated hematologic process is referred to as Evans Syndrome (ES), named after Dr. Robert Evans who in 1951 first described the association of the former two diagnoses [<span>1</span>]. The eponym was then extended to include the possibility of AIN in the 1990s, a diagnosis with pathophysiology suggestive of the causal involvement of antineutrophil antibodies in 1975 [<span>2</span>].</p><p>The 2023 treatment considerations for AIN, when treatment is needed, include granulocyte-colony stimulating factor and/or immunosuppression, whereas the recommended first- and second-line treatment paradigms for ITP, wAIHA, and ES include immunosuppression anchored on corticosteroids and the monoclonal anti-CD20 rituximab, with additional consideration in the case of ITP for thrombopoietic agents referred to as thrombopoietin receptor agonists [<span>3-6</span>]. Third-line treatment includes additional immunosuppressant considerations, such as azathioprine and cyclosporine, and most recently, splenectomy, as a now-downgraded (i.e., third-line) therapeutic modality [<span>4-6</span>].</p><p>For ITP and wAIHA, and by extension their overlap known as ES, splenectomy was the preferred second-line treatment for over 50 years through the 2010s, being recommended by leading experts as recently as 2010 and 2011 for AIHA and ITP, respectively [<span>7, 8</span>]. As experience with the off-label use of rituximab grew, splenectomy increasingly drifted toward third-line treatment status due to concern of the tripartite risk of infection, thrombosis, and perioperative mortality [<span>4, 6</span>]. The point estimates for these risks, however, date to the 1990s and 2000s, and so predate advances in preoperative vaccination, thromboprophylaxis, and the laparoscopic approach to splenectomy. Nevertheless, and without the quantification of total splenectomy risk through the 2010s, splenectomy-associated risks have been qualitatively noted as likely too great. In our experience at the bedside, this has led to questions of appropriate patient counseling and informed consent. This is especially the case for individuals whose values and preferences align with pursuing a potentially one-time, definitive treatment, but who are dissuaded from pursuing splenectomy because the “risks are too great.” The issue does not exist on a population level, where we know that splenectomy continues to be the therapeutic modality with the highest probability of documented, long-term effectiveness without need for continuous therapy. Rather, the issue exists at the crucial individual level, where clinicians worry that we often cannot adequately adjust the pretest probability for the risk of disease recurrence after splenectomy for individual patients. Due to both ethical and practical considerations, we will never have prospective, randomized trial data to make these decisions. And yet these decisions need to be made, ideally with consent that is as informed as data limitations ultimately allow.</p><p>It is in this context of the absence of planned prospective data collection in this arena that, in this issue of the <i>Journal of Internal Medicine</i>, Ogbue et al. provide crucial insights of their institutional experience with splenectomy in the treatment of patients with a variety of autoimmune cytopenias at the Cleveland Clinic, an institution in the United States with a deep commitment to clinical excellence [<span>9</span>]. The authors meticulously applied thoughtful exclusion criteria through a retrospective evaluation of 1824 consecutive splenectomy cases across the years 2002–2020 to properly isolate 339 patients who underwent splenectomy for one of the following autoimmune cytopenia diagnoses with a subsequent median follow-up of 5 years: ITP (<i>n</i> = 235), AIHA (<i>n</i> = 68), ES (<i>n</i> = 26), and AIN (<i>n</i> = 10). Of particular importance, they report (1) appropriately adjudicated (i.e., disease-definition-specific) response and relapse rates at each yearly interval of follow-up for each autoimmune cytopenia; (2) complication rates accrued in per person-years for infection, thrombosis, and mortality; (3) patient vaccination status; (4) postoperative complications; and (5) pathology-proven discordant diagnoses appropriately removed from effectiveness metrics (Fig. 1). The authors additionally utilized their sample size to perform logistic regression across an appropriate maximum amount of risk factors to identify covariates that may be associated with favorable and unfavorable response to splenectomy.</p><p>Specifically, the authors report a robust 74% overall hematologic response rate with a 12% relapse rate; rates that have historically been expected with splenectomy across cohorts of individuals with the considered autoimmune cytopenias. Additionally, surgical complication rates and long-term morbidity were low, and this is despite a patient cohort that appears to be notably under-vaccinated for splenectomy, an issue that has been noted previously in modern medicine [<span>10</span>]. The authors attempted to identify key clinical covariates that are associated with both favorable and unfavorable responses to splenectomy. Although several were identified on univariable analyses, multivariable regression identified preoperative refractoriness or relapse after multiple lines of therapy as associated with splenectomy treatment failure. Arguably the most striking aspect of their study lies in their reporting of the value added of splenectomy as a diagnostic tool, in addition to its therapeutic potency. In 13% of all patients who underwent splenectomy, tissue diagnosis yielded a diagnosis that was discordant from the working diagnosis prior to splenectomy. The correct diagnoses largely included a variety of malignancies that have entirely different treatment paradigms, with most representing different types of lymphoma, which are notorious for difficulty of diagnosis when confined to the spleen and are known to drive immune-mediated hematologic findings that can resemble some autoimmune cytopenias.</p><p>Ogbue et al. are to be commended for conducting a rigorous retrospective analysis across heterogeneous conditions in a way that has added value to the field for patients and physicians. These findings buttress an increasing base of information within an important knowledge gap regarding splenectomy risks, the presence of which over the years has convinced some of our patients to stay away from splenectomy without properly informed consent. The authors also showcase the additional value of splenectomy for patients in making the correct diagnosis, even in the context of an institution known globally for clinical excellence. As important, properly reported rates in per-person-years of this well-annotated cohort provide a bevy of information that will be useful to researchers in health decision science and separately for researchers who may opt to pursue the creation of a patient decision aid in this space. Most important, it provides a well-done study beyond the ITP arena, with an additional focus on wAIHA and ES, that will incrementally help improve patient–physician shared decision-making in these treatment arenas.</p><p>As with all retrospective analyses, however, there are notable limitations. The work, in its nature, cannot be predictive. The sample sizes, although superb for rare disease work, are also relatively small, and the diseases under study are notably heterogeneous. Similar work at other institutions, particularly for diseases other than primary ITP, where there is substantially more data than in wAIHA and ES, would be helpful to confirm the effectiveness data. Most important, our patients are making a lifelong, unalterable decision when it comes to pursuing splenectomy, and so data well beyond a median follow-up of 5 years is needed. Thankfully, we now have data out to 20 years in ITP in at least one report, but similar data is lacking for wAIHA and ES. In addition, no generalizable conclusions should be drawn on the effectiveness of splenectomy for individuals with AIN given the very small sample size. Finally, the identified covariates associated with response, or lack thereof, to splenectomy are important confirmations and are not novel for practicing clinicians: The issue regarding uncertainty for patient selection for the splenectomy modality will continue.</p><p>Nevertheless, despite the limitations and even in the context of wonderful non-surgical therapeutic options, Ogbue et al. add sufficient data to remind us that splenectomy as a third-line option is inappropriate for all patients with autoimmune cytopenias. They additionally provide new data as to the risk of postsplenectomy infection while noting that the period under study does not exclusively span the modern vaccination era and that many patients may have been notably under-vaccinated. These are opportunities for the field and for our patients. As we continue to re-appraise the value of splenectomy, we need to ensure that all patients opting for the <i>possibility</i> of definitive, one-time treatment receive all recommended vaccinations and undergo appropriate discussion and risk stratification that considers their individual-specific covariates when it comes to thromboprophylaxis and the surgical approach. This would allow a true alignment of clinical care with patient values and preferences, in the context of known uncertainty and expected comparative data limitations when it comes to splenectomy consideration for all individuals living with autoimmune cytopenias.</p><p>The authors have no conflicts of interest to declare.</p>\",\"PeriodicalId\":196,\"journal\":{\"name\":\"Journal of Internal Medicine\",\"volume\":\"295 2\",\"pages\":\"120-122\"},\"PeriodicalIF\":9.2000,\"publicationDate\":\"2023-12-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.13756\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Internal Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/joim.13756\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.13756","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
具体来说,作者报告的总体血液学反应率高达 74%,复发率为 12%;这一比率在患有自身免疫性细胞减少症的人群中历来是脾切除术的预期目标。此外,手术并发症发生率和长期发病率都很低,尽管患者队列中脾切除术的疫苗接种似乎明显不足,但这一问题在现代医学中已被注意到[10]。作者试图找出与脾切除术有利和不利反应相关的关键临床协变量。虽然在单变量分析中发现了几个变量,但多变量回归发现术前难治性或多线治疗后复发与脾切除术治疗失败有关。可以说,他们的研究中最引人注目的地方在于,他们报告了脾切除术除了具有治疗作用外,还作为一种诊断工具带来的附加值。在所有接受脾切除术的患者中,有 13% 的组织诊断结果与脾切除术前的工作诊断结果不一致。正确的诊断主要包括治疗模式完全不同的各种恶性肿瘤,其中大多数代表不同类型的淋巴瘤,当淋巴瘤局限于脾脏时很难诊断,众所周知,淋巴瘤会导致免疫介导的血液学结果,这可能类似于一些自身免疫性细胞减少症。Ogbue 等人对异质性疾病进行了严格的回顾性分析,为该领域的患者和医生增加了价值,值得称赞。这些研究结果加强了有关脾切除术风险的重要知识缺口的信息基础,多年来,这些风险的存在使我们的一些患者在未获得适当知情同意的情况下远离脾切除术。作者还展示了脾脏切除术对患者做出正确诊断的额外价值,即使是在以临床卓越而闻名全球的医疗机构中也是如此。同样重要的是,在这个经过精心注释的队列中,以每人每年为单位的正确报告率提供了大量信息,这些信息对健康决策科学的研究人员很有帮助,对可能选择在这一领域创建患者决策辅助工具的研究人员也很有帮助。最重要的是,它提供了一项超越 ITP 领域的精心研究,并额外关注了 wAIHA 和 ES,这将有助于逐步改善这些治疗领域的患者-医生共同决策。就其本质而言,这项工作不具有预测性。样本量虽然在罕见病研究中堪称一流,但也相对较小,而且所研究的疾病具有明显的异质性。其他机构开展的类似工作,尤其是针对原发性 ITP 以外疾病的工作,将有助于证实有效性数据,因为这些疾病的数据远远多于 wAIHA 和 ES 的数据。最重要的是,我们的患者在接受脾切除术时做出了终生不可改变的决定,因此需要远超中位随访 5 年的数据。值得庆幸的是,现在至少有一份报告提供了 ITP 长达 20 年的数据,但 wAIHA 和 ES 还缺乏类似的数据。此外,由于样本量非常小,因此对于 AIN 患者进行脾切除术的有效性,还不能得出具有普遍意义的结论。最后,已确定的与脾切除术反应或无反应相关的协变量是重要的确认因素,对临床医生来说并不陌生:然而,尽管存在这些局限性,甚至在非手术治疗选择非常好的情况下,Ogbue 等人的研究仍提供了足够的数据来提醒我们,脾切除术作为三线治疗方案并不适用于所有自身免疫性细胞减少症患者。此外,他们还就脾切除术后感染的风险提供了新数据,同时指出研究期间并不完全是现代疫苗接种时代,许多患者的疫苗接种可能明显不足。这些对本领域和我们的患者来说都是机遇。当我们继续重新评估脾切除术的价值时,我们需要确保所有选择接受一次性明确治疗的患者都接受了所有推荐的疫苗接种,并进行了适当的讨论和风险分层,在涉及血栓预防和手术方法时考虑到了他们的个体特异性协变量。在所有自身免疫性细胞减少症患者考虑脾切除术时,由于已知的不确定性和预期比较数据的局限性,这将使临床治疗真正符合患者的价值观和偏好。
Splenectomy reappraised: Bridging the gap in immune cytopenia treatment paradigms
The spleen is often the primary site of autoantibody production and autoantibody-coated clearance of hematologic cells in several immune-mediated hematologic rare diseases collectively referred to as autoimmune cytopenias. The affected hematologic cell lines in autoimmune cytopenia disorders most commonly include platelets, red cells, and neutrophils, with the respective conditions referred to as immune thrombocytopenic purpura (ITP), warm autoimmune hemolytic anemia (wAIHA), and autoimmune neutropenia (AIN). When two of these conditions co-occur, the immune-mediated hematologic process is referred to as Evans Syndrome (ES), named after Dr. Robert Evans who in 1951 first described the association of the former two diagnoses [1]. The eponym was then extended to include the possibility of AIN in the 1990s, a diagnosis with pathophysiology suggestive of the causal involvement of antineutrophil antibodies in 1975 [2].
The 2023 treatment considerations for AIN, when treatment is needed, include granulocyte-colony stimulating factor and/or immunosuppression, whereas the recommended first- and second-line treatment paradigms for ITP, wAIHA, and ES include immunosuppression anchored on corticosteroids and the monoclonal anti-CD20 rituximab, with additional consideration in the case of ITP for thrombopoietic agents referred to as thrombopoietin receptor agonists [3-6]. Third-line treatment includes additional immunosuppressant considerations, such as azathioprine and cyclosporine, and most recently, splenectomy, as a now-downgraded (i.e., third-line) therapeutic modality [4-6].
For ITP and wAIHA, and by extension their overlap known as ES, splenectomy was the preferred second-line treatment for over 50 years through the 2010s, being recommended by leading experts as recently as 2010 and 2011 for AIHA and ITP, respectively [7, 8]. As experience with the off-label use of rituximab grew, splenectomy increasingly drifted toward third-line treatment status due to concern of the tripartite risk of infection, thrombosis, and perioperative mortality [4, 6]. The point estimates for these risks, however, date to the 1990s and 2000s, and so predate advances in preoperative vaccination, thromboprophylaxis, and the laparoscopic approach to splenectomy. Nevertheless, and without the quantification of total splenectomy risk through the 2010s, splenectomy-associated risks have been qualitatively noted as likely too great. In our experience at the bedside, this has led to questions of appropriate patient counseling and informed consent. This is especially the case for individuals whose values and preferences align with pursuing a potentially one-time, definitive treatment, but who are dissuaded from pursuing splenectomy because the “risks are too great.” The issue does not exist on a population level, where we know that splenectomy continues to be the therapeutic modality with the highest probability of documented, long-term effectiveness without need for continuous therapy. Rather, the issue exists at the crucial individual level, where clinicians worry that we often cannot adequately adjust the pretest probability for the risk of disease recurrence after splenectomy for individual patients. Due to both ethical and practical considerations, we will never have prospective, randomized trial data to make these decisions. And yet these decisions need to be made, ideally with consent that is as informed as data limitations ultimately allow.
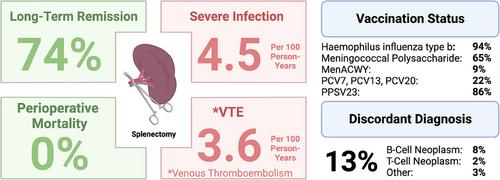
It is in this context of the absence of planned prospective data collection in this arena that, in this issue of the Journal of Internal Medicine, Ogbue et al. provide crucial insights of their institutional experience with splenectomy in the treatment of patients with a variety of autoimmune cytopenias at the Cleveland Clinic, an institution in the United States with a deep commitment to clinical excellence [9]. The authors meticulously applied thoughtful exclusion criteria through a retrospective evaluation of 1824 consecutive splenectomy cases across the years 2002–2020 to properly isolate 339 patients who underwent splenectomy for one of the following autoimmune cytopenia diagnoses with a subsequent median follow-up of 5 years: ITP (n = 235), AIHA (n = 68), ES (n = 26), and AIN (n = 10). Of particular importance, they report (1) appropriately adjudicated (i.e., disease-definition-specific) response and relapse rates at each yearly interval of follow-up for each autoimmune cytopenia; (2) complication rates accrued in per person-years for infection, thrombosis, and mortality; (3) patient vaccination status; (4) postoperative complications; and (5) pathology-proven discordant diagnoses appropriately removed from effectiveness metrics (Fig. 1). The authors additionally utilized their sample size to perform logistic regression across an appropriate maximum amount of risk factors to identify covariates that may be associated with favorable and unfavorable response to splenectomy.
Specifically, the authors report a robust 74% overall hematologic response rate with a 12% relapse rate; rates that have historically been expected with splenectomy across cohorts of individuals with the considered autoimmune cytopenias. Additionally, surgical complication rates and long-term morbidity were low, and this is despite a patient cohort that appears to be notably under-vaccinated for splenectomy, an issue that has been noted previously in modern medicine [10]. The authors attempted to identify key clinical covariates that are associated with both favorable and unfavorable responses to splenectomy. Although several were identified on univariable analyses, multivariable regression identified preoperative refractoriness or relapse after multiple lines of therapy as associated with splenectomy treatment failure. Arguably the most striking aspect of their study lies in their reporting of the value added of splenectomy as a diagnostic tool, in addition to its therapeutic potency. In 13% of all patients who underwent splenectomy, tissue diagnosis yielded a diagnosis that was discordant from the working diagnosis prior to splenectomy. The correct diagnoses largely included a variety of malignancies that have entirely different treatment paradigms, with most representing different types of lymphoma, which are notorious for difficulty of diagnosis when confined to the spleen and are known to drive immune-mediated hematologic findings that can resemble some autoimmune cytopenias.
Ogbue et al. are to be commended for conducting a rigorous retrospective analysis across heterogeneous conditions in a way that has added value to the field for patients and physicians. These findings buttress an increasing base of information within an important knowledge gap regarding splenectomy risks, the presence of which over the years has convinced some of our patients to stay away from splenectomy without properly informed consent. The authors also showcase the additional value of splenectomy for patients in making the correct diagnosis, even in the context of an institution known globally for clinical excellence. As important, properly reported rates in per-person-years of this well-annotated cohort provide a bevy of information that will be useful to researchers in health decision science and separately for researchers who may opt to pursue the creation of a patient decision aid in this space. Most important, it provides a well-done study beyond the ITP arena, with an additional focus on wAIHA and ES, that will incrementally help improve patient–physician shared decision-making in these treatment arenas.
As with all retrospective analyses, however, there are notable limitations. The work, in its nature, cannot be predictive. The sample sizes, although superb for rare disease work, are also relatively small, and the diseases under study are notably heterogeneous. Similar work at other institutions, particularly for diseases other than primary ITP, where there is substantially more data than in wAIHA and ES, would be helpful to confirm the effectiveness data. Most important, our patients are making a lifelong, unalterable decision when it comes to pursuing splenectomy, and so data well beyond a median follow-up of 5 years is needed. Thankfully, we now have data out to 20 years in ITP in at least one report, but similar data is lacking for wAIHA and ES. In addition, no generalizable conclusions should be drawn on the effectiveness of splenectomy for individuals with AIN given the very small sample size. Finally, the identified covariates associated with response, or lack thereof, to splenectomy are important confirmations and are not novel for practicing clinicians: The issue regarding uncertainty for patient selection for the splenectomy modality will continue.
Nevertheless, despite the limitations and even in the context of wonderful non-surgical therapeutic options, Ogbue et al. add sufficient data to remind us that splenectomy as a third-line option is inappropriate for all patients with autoimmune cytopenias. They additionally provide new data as to the risk of postsplenectomy infection while noting that the period under study does not exclusively span the modern vaccination era and that many patients may have been notably under-vaccinated. These are opportunities for the field and for our patients. As we continue to re-appraise the value of splenectomy, we need to ensure that all patients opting for the possibility of definitive, one-time treatment receive all recommended vaccinations and undergo appropriate discussion and risk stratification that considers their individual-specific covariates when it comes to thromboprophylaxis and the surgical approach. This would allow a true alignment of clinical care with patient values and preferences, in the context of known uncertainty and expected comparative data limitations when it comes to splenectomy consideration for all individuals living with autoimmune cytopenias.
The authors have no conflicts of interest to declare.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
