Ankia Coetzee, David R Hall, Eduard J Langenegger, Mari van de Vyver, Magda Conradie
{"title":"妊娠与糖尿病酮症酸中毒:胎儿危险和机会之窗。","authors":"Ankia Coetzee, David R Hall, Eduard J Langenegger, Mari van de Vyver, Magda Conradie","doi":"10.3389/fcdhc.2023.1266017","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetic ketoacidosis (DKA) during pregnancy poses significant risks to both the mother and fetus, with an increased risk of fetal demise. Although more prevalent in women with Type I diabetes (T1D); those with Type 2 diabetes (T2D) and gestational diabetes mellitus (GDM) can also develop DKA. A lack of information about DKA during pregnancy exists worldwide, including in South Africa.</p><p><strong>Objective: </strong>This study examined the characteristics and outcomes associated with DKA during pregnancy.</p><p><strong>Methods: </strong>The study took place between 1 April 2020 and 1 October 2022. Pregnant women with DKA, admitted to Tygerberg Hospital's Obstetric Critical Care Unit (OCCU) were included. Maternal characteristics, precipitants of DKA, adverse events during treatment, and maternal-fetal outcomes were examined.</p><p><strong>Results: </strong>There were 54 episodes of DKA among 47 women. Most DKA's were mild and occurred in the third trimester. Pregestational diabetes dominated (31/47; 60%), with 47% having T1D and 94% requiring insulin. Seven women (7/47, 15%; T2D:6, T1D:1) had two episodes of DKA during the same pregnancy. Most women (32/47; 68%) were either overweight or obese. Yet, despite the T2D phenotype, biomarkers indicated that auto-immune diabetes was prevalent among women without any prior history of T1D (6/21; 29%). Twelve women (26%) developed gestational hypertension during pregnancy, and 17 (36%) pre-eclampsia. Precipitating causes of DKA included infection (14/54; 26%), insulin disruption (14/54; 26%) and betamethasone administration (10/54; 19%). More than half of the episodes of DKA involved hypokalemia (35/54, 65%) that was associated with fetal death (P=0.042) and hypoglycemia (28/54, 52%). Preterm birth (<37 weeks' gestation) occurred in 85% of women. No maternal deaths were recorded. A high fetal mortality rate (13/47; 28%) that included 11 spontaneous intrauterine deaths and two medical terminations, was observed.</p><p><strong>Conclusion: </strong>Women with DKA have a high risk of fetal mortality as well as undiagnosed auto-immune diabetes. There is a strong link between maternal hypokalemia and fetal loss, suggesting an opportunity to address management gaps in pregnant women with DKA.</p>","PeriodicalId":73075,"journal":{"name":"Frontiers in clinical diabetes and healthcare","volume":"4 ","pages":"1266017"},"PeriodicalIF":2.2000,"publicationDate":"2023-11-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10693403/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pregnancy and diabetic ketoacidosis: fetal jeopardy and windows of opportunity.\",\"authors\":\"Ankia Coetzee, David R Hall, Eduard J Langenegger, Mari van de Vyver, Magda Conradie\",\"doi\":\"10.3389/fcdhc.2023.1266017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Diabetic ketoacidosis (DKA) during pregnancy poses significant risks to both the mother and fetus, with an increased risk of fetal demise. Although more prevalent in women with Type I diabetes (T1D); those with Type 2 diabetes (T2D) and gestational diabetes mellitus (GDM) can also develop DKA. A lack of information about DKA during pregnancy exists worldwide, including in South Africa.</p><p><strong>Objective: </strong>This study examined the characteristics and outcomes associated with DKA during pregnancy.</p><p><strong>Methods: </strong>The study took place between 1 April 2020 and 1 October 2022. Pregnant women with DKA, admitted to Tygerberg Hospital's Obstetric Critical Care Unit (OCCU) were included. Maternal characteristics, precipitants of DKA, adverse events during treatment, and maternal-fetal outcomes were examined.</p><p><strong>Results: </strong>There were 54 episodes of DKA among 47 women. Most DKA's were mild and occurred in the third trimester. Pregestational diabetes dominated (31/47; 60%), with 47% having T1D and 94% requiring insulin. Seven women (7/47, 15%; T2D:6, T1D:1) had two episodes of DKA during the same pregnancy. Most women (32/47; 68%) were either overweight or obese. Yet, despite the T2D phenotype, biomarkers indicated that auto-immune diabetes was prevalent among women without any prior history of T1D (6/21; 29%). Twelve women (26%) developed gestational hypertension during pregnancy, and 17 (36%) pre-eclampsia. Precipitating causes of DKA included infection (14/54; 26%), insulin disruption (14/54; 26%) and betamethasone administration (10/54; 19%). More than half of the episodes of DKA involved hypokalemia (35/54, 65%) that was associated with fetal death (P=0.042) and hypoglycemia (28/54, 52%). Preterm birth (<37 weeks' gestation) occurred in 85% of women. No maternal deaths were recorded. A high fetal mortality rate (13/47; 28%) that included 11 spontaneous intrauterine deaths and two medical terminations, was observed.</p><p><strong>Conclusion: </strong>Women with DKA have a high risk of fetal mortality as well as undiagnosed auto-immune diabetes. There is a strong link between maternal hypokalemia and fetal loss, suggesting an opportunity to address management gaps in pregnant women with DKA.</p>\",\"PeriodicalId\":73075,\"journal\":{\"name\":\"Frontiers in clinical diabetes and healthcare\",\"volume\":\"4 \",\"pages\":\"1266017\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-11-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10693403/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in clinical diabetes and healthcare\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fcdhc.2023.1266017\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in clinical diabetes and healthcare","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fcdhc.2023.1266017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Pregnancy and diabetic ketoacidosis: fetal jeopardy and windows of opportunity.
Background: Diabetic ketoacidosis (DKA) during pregnancy poses significant risks to both the mother and fetus, with an increased risk of fetal demise. Although more prevalent in women with Type I diabetes (T1D); those with Type 2 diabetes (T2D) and gestational diabetes mellitus (GDM) can also develop DKA. A lack of information about DKA during pregnancy exists worldwide, including in South Africa.
Objective: This study examined the characteristics and outcomes associated with DKA during pregnancy.
Methods: The study took place between 1 April 2020 and 1 October 2022. Pregnant women with DKA, admitted to Tygerberg Hospital's Obstetric Critical Care Unit (OCCU) were included. Maternal characteristics, precipitants of DKA, adverse events during treatment, and maternal-fetal outcomes were examined.
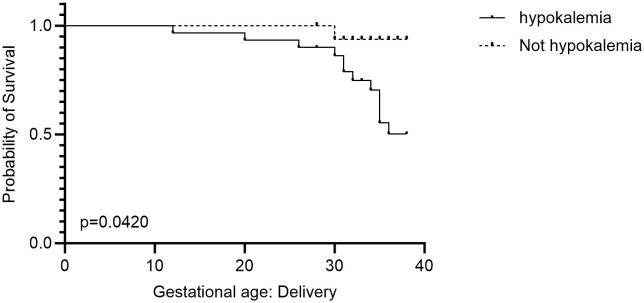
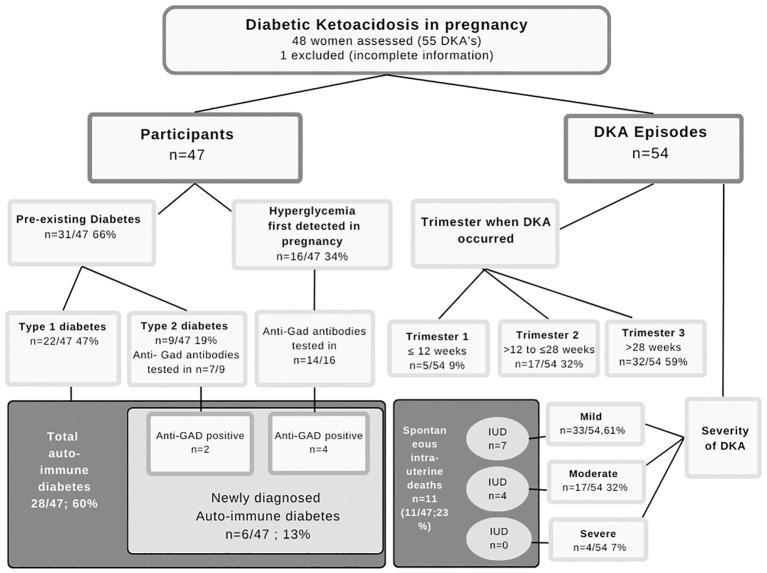
Results: There were 54 episodes of DKA among 47 women. Most DKA's were mild and occurred in the third trimester. Pregestational diabetes dominated (31/47; 60%), with 47% having T1D and 94% requiring insulin. Seven women (7/47, 15%; T2D:6, T1D:1) had two episodes of DKA during the same pregnancy. Most women (32/47; 68%) were either overweight or obese. Yet, despite the T2D phenotype, biomarkers indicated that auto-immune diabetes was prevalent among women without any prior history of T1D (6/21; 29%). Twelve women (26%) developed gestational hypertension during pregnancy, and 17 (36%) pre-eclampsia. Precipitating causes of DKA included infection (14/54; 26%), insulin disruption (14/54; 26%) and betamethasone administration (10/54; 19%). More than half of the episodes of DKA involved hypokalemia (35/54, 65%) that was associated with fetal death (P=0.042) and hypoglycemia (28/54, 52%). Preterm birth (<37 weeks' gestation) occurred in 85% of women. No maternal deaths were recorded. A high fetal mortality rate (13/47; 28%) that included 11 spontaneous intrauterine deaths and two medical terminations, was observed.
Conclusion: Women with DKA have a high risk of fetal mortality as well as undiagnosed auto-immune diabetes. There is a strong link between maternal hypokalemia and fetal loss, suggesting an opportunity to address management gaps in pregnant women with DKA.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
