{"title":"用生物制剂治疗 IgA 肾病的进展","authors":"Yongze Zhuang, Hailing Lu, Junxia Li","doi":"10.1002/cdt3.104","DOIUrl":null,"url":null,"abstract":"<p>Immunoglobulin A nephropathy (IgAN) is the most common primary glomerular disease, and the “four-hit” theory represents its currently accepted pathogenic mechanism. Mucosal immunity triggered by infections in the respiratory tract, intestines, or other areas leads to antigen presentation, T cell stimulation, B cell maturation, and the production of IgA-producing plasma cells. The proteins B-lymphocyte stimulator (BLyS) and a proliferation-inducing ligand (APRIL) are involved in this process, and alternative complement and lectin pathway activation are also part of the pathogenic mechanism. Kidney Disease Improving Global Outcomes guidelines indicate that a specific effective treatment for IgAN is lacking, with renin–angiotensin–aldosterone system inhibitors being the primary therapy. Recent research shows that biological agents can significantly reduce proteinuria, stabilize the estimated glomerular filtration rate, and reverse some pathological changes, such as endocapillary proliferation and crescent formation. There are four main categories of biological agents used to treat IgA nephropathy, specifically anti-CD20 monoclonal antibodies, anti-BLyS or APRIL monoclonal antibodies, monoclonal antibodies targeting both BLyS and APRIL (telitacicept and atacicept), and monoclonal antibodies inhibiting complement system activation (narsoplimab and eculizumab). However, further research on the dosages, treatment duration, long-term efficacy, and safety of these biological agents is required.</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"10 1","pages":"1-11"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cdt3.104","citationCount":"0","resultStr":"{\"title\":\"Advances in the treatment of IgA nephropathy with biological agents\",\"authors\":\"Yongze Zhuang, Hailing Lu, Junxia Li\",\"doi\":\"10.1002/cdt3.104\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Immunoglobulin A nephropathy (IgAN) is the most common primary glomerular disease, and the “four-hit” theory represents its currently accepted pathogenic mechanism. Mucosal immunity triggered by infections in the respiratory tract, intestines, or other areas leads to antigen presentation, T cell stimulation, B cell maturation, and the production of IgA-producing plasma cells. The proteins B-lymphocyte stimulator (BLyS) and a proliferation-inducing ligand (APRIL) are involved in this process, and alternative complement and lectin pathway activation are also part of the pathogenic mechanism. Kidney Disease Improving Global Outcomes guidelines indicate that a specific effective treatment for IgAN is lacking, with renin–angiotensin–aldosterone system inhibitors being the primary therapy. Recent research shows that biological agents can significantly reduce proteinuria, stabilize the estimated glomerular filtration rate, and reverse some pathological changes, such as endocapillary proliferation and crescent formation. There are four main categories of biological agents used to treat IgA nephropathy, specifically anti-CD20 monoclonal antibodies, anti-BLyS or APRIL monoclonal antibodies, monoclonal antibodies targeting both BLyS and APRIL (telitacicept and atacicept), and monoclonal antibodies inhibiting complement system activation (narsoplimab and eculizumab). However, further research on the dosages, treatment duration, long-term efficacy, and safety of these biological agents is required.</p>\",\"PeriodicalId\":32096,\"journal\":{\"name\":\"Chronic Diseases and Translational Medicine\",\"volume\":\"10 1\",\"pages\":\"1-11\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-12-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cdt3.104\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chronic Diseases and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.104\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.104","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
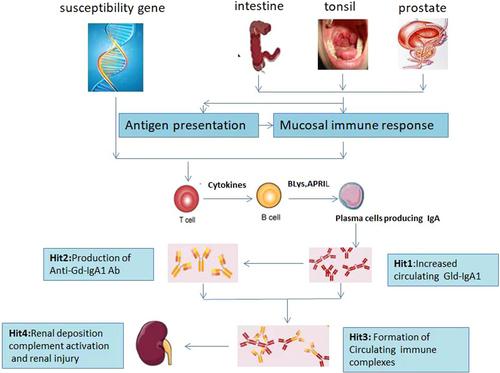
免疫球蛋白 A 肾病(IgAN)是最常见的原发性肾小球疾病,"四击 "理论是目前公认的致病机制。呼吸道、肠道或其他部位的感染引发的粘膜免疫会导致抗原呈递、T 细胞刺激、B 细胞成熟和产生 IgA 的浆细胞。蛋白质 B 淋巴细胞刺激素(BLyS)和增殖诱导配体(APRIL)参与了这一过程,替代性补体和凝集素通路激活也是致病机制的一部分。肾脏病改善全球结果指南》指出,目前还缺乏治疗 IgAN 的有效特效药物,主要疗法是肾素-血管紧张素-醛固酮系统抑制剂。最近的研究表明,生物制剂可以显著减少蛋白尿,稳定肾小球滤过率,并逆转一些病理变化,如毛细血管内膜增生和新月体形成。用于治疗 IgA 肾病的生物制剂主要有四大类,即抗 CD20 单克隆抗体、抗 BLyS 或 APRIL 单克隆抗体、同时针对 BLyS 和 APRIL 的单克隆抗体(telitacicept 和 atacicept)以及抑制补体系统激活的单克隆抗体(narsoplimab 和 eculizumab)。然而,还需要对这些生物制剂的剂量、疗程、长期疗效和安全性进行进一步研究。
Advances in the treatment of IgA nephropathy with biological agents
Immunoglobulin A nephropathy (IgAN) is the most common primary glomerular disease, and the “four-hit” theory represents its currently accepted pathogenic mechanism. Mucosal immunity triggered by infections in the respiratory tract, intestines, or other areas leads to antigen presentation, T cell stimulation, B cell maturation, and the production of IgA-producing plasma cells. The proteins B-lymphocyte stimulator (BLyS) and a proliferation-inducing ligand (APRIL) are involved in this process, and alternative complement and lectin pathway activation are also part of the pathogenic mechanism. Kidney Disease Improving Global Outcomes guidelines indicate that a specific effective treatment for IgAN is lacking, with renin–angiotensin–aldosterone system inhibitors being the primary therapy. Recent research shows that biological agents can significantly reduce proteinuria, stabilize the estimated glomerular filtration rate, and reverse some pathological changes, such as endocapillary proliferation and crescent formation. There are four main categories of biological agents used to treat IgA nephropathy, specifically anti-CD20 monoclonal antibodies, anti-BLyS or APRIL monoclonal antibodies, monoclonal antibodies targeting both BLyS and APRIL (telitacicept and atacicept), and monoclonal antibodies inhibiting complement system activation (narsoplimab and eculizumab). However, further research on the dosages, treatment duration, long-term efficacy, and safety of these biological agents is required.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
