Tsugumi Satoh, Hidekazu Kayano, Mika Kohri, Ken Tanae, Chie Asou, Naoki Takahashi, Kunihiro Tsukasaki, Masanori Yasuda
{"title":"新发T淋巴细胞淋巴瘤和皮肤γ/δ外周T细胞淋巴瘤的并发症。","authors":"Tsugumi Satoh, Hidekazu Kayano, Mika Kohri, Ken Tanae, Chie Asou, Naoki Takahashi, Kunihiro Tsukasaki, Masanori Yasuda","doi":"10.3960/jslrt.23042","DOIUrl":null,"url":null,"abstract":"<p><p>The coincidence of acute T-lymphoblastic leukemia/lymphoma, NOS (T-ALL/LBL), and peripheral T-cell lymphoma (PTCL) is unusual, and there have only been a few cases of their metachronous occurrence. In these cases, PTCLs emerged as recurrence after primary therapy for primary T-ALL, were the rare gamma/delta type, and uncommonly involved skin for T-ALL/LBL. We herein report the first case of de novo T-LBL that coincided with cutaneous gamma/delta PTCL before primary therapy. A 70-year-old man presented with systemic lymphadenopathy. Lymph node biopsy revealed a massive proliferation of lymphoblastoid cells; immunohistochemically, they were positive for TdT/CD1a/CD99, and cytoplasmic CD3ε, CD4, and CD8 and were negative for T-cell receptor (TCR) βf-1. A few TCRδ-positive cells were intermingled. Atypically, TIA was focally positive, whereas granzyme/perforin was negative. Multiple papules and plaques emerged on the trunk before the initiation of treatment for T-LBL. Skin biopsy revealed a massive proliferation of medium-to-large atypical lymphoid cells that were TdT/CD1a-negative mature T-cells; they were negative for TCRβf1 and CD4, and positive for TCRδ, CD5, CD8, CD56, TIA, granzyme B, and perforin. A conventional PCR analysis of TCRG showed no identical clonal band between the two tumors. The skin lesion was diagnosed as cutaneous gamma/delta T-cell lymphoma. Whether the lesion was primary or a transformation of T-LBL was unclear. After treating with reduced hyper-CVAD/MA targeting T-LBL, molecular complete remission was achieved. When an uncommon cutaneous lesion emerges in the course of T-ALL/LBL, both need to be evaluated pathologically and genetically, whether de novo or recurrent, assuming the possibility of coincident gamma/delta PTCL.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":"63 4","pages":"257-261"},"PeriodicalIF":1.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10861366/pdf/","citationCount":"0","resultStr":"{\"title\":\"Coincidence of de novo T-lymphoblastic lymphoma and cutaneous gamma/delta peripheral T-cell lymphoma.\",\"authors\":\"Tsugumi Satoh, Hidekazu Kayano, Mika Kohri, Ken Tanae, Chie Asou, Naoki Takahashi, Kunihiro Tsukasaki, Masanori Yasuda\",\"doi\":\"10.3960/jslrt.23042\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The coincidence of acute T-lymphoblastic leukemia/lymphoma, NOS (T-ALL/LBL), and peripheral T-cell lymphoma (PTCL) is unusual, and there have only been a few cases of their metachronous occurrence. In these cases, PTCLs emerged as recurrence after primary therapy for primary T-ALL, were the rare gamma/delta type, and uncommonly involved skin for T-ALL/LBL. We herein report the first case of de novo T-LBL that coincided with cutaneous gamma/delta PTCL before primary therapy. A 70-year-old man presented with systemic lymphadenopathy. Lymph node biopsy revealed a massive proliferation of lymphoblastoid cells; immunohistochemically, they were positive for TdT/CD1a/CD99, and cytoplasmic CD3ε, CD4, and CD8 and were negative for T-cell receptor (TCR) βf-1. A few TCRδ-positive cells were intermingled. Atypically, TIA was focally positive, whereas granzyme/perforin was negative. Multiple papules and plaques emerged on the trunk before the initiation of treatment for T-LBL. Skin biopsy revealed a massive proliferation of medium-to-large atypical lymphoid cells that were TdT/CD1a-negative mature T-cells; they were negative for TCRβf1 and CD4, and positive for TCRδ, CD5, CD8, CD56, TIA, granzyme B, and perforin. A conventional PCR analysis of TCRG showed no identical clonal band between the two tumors. The skin lesion was diagnosed as cutaneous gamma/delta T-cell lymphoma. Whether the lesion was primary or a transformation of T-LBL was unclear. After treating with reduced hyper-CVAD/MA targeting T-LBL, molecular complete remission was achieved. When an uncommon cutaneous lesion emerges in the course of T-ALL/LBL, both need to be evaluated pathologically and genetically, whether de novo or recurrent, assuming the possibility of coincident gamma/delta PTCL.</p>\",\"PeriodicalId\":45936,\"journal\":{\"name\":\"Journal of Clinical and Experimental Hematopathology\",\"volume\":\"63 4\",\"pages\":\"257-261\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10861366/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Experimental Hematopathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3960/jslrt.23042\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.23042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
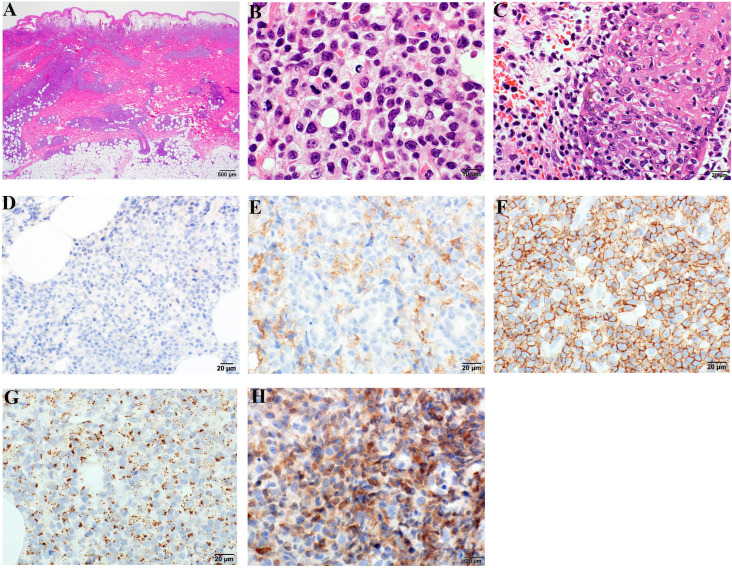
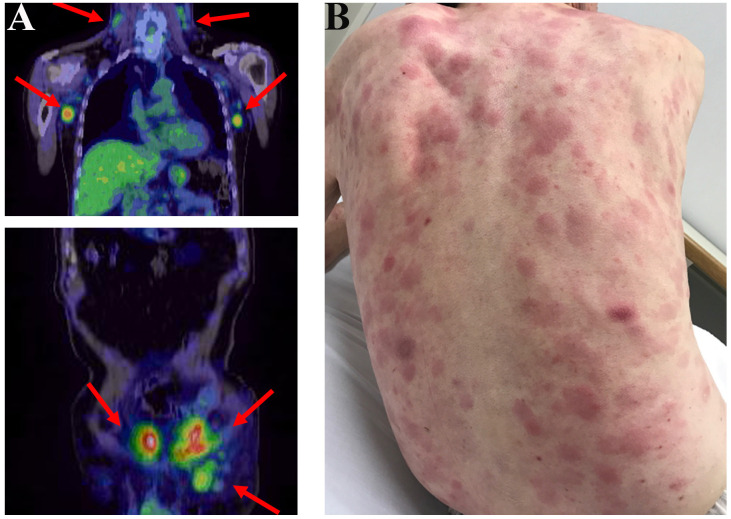
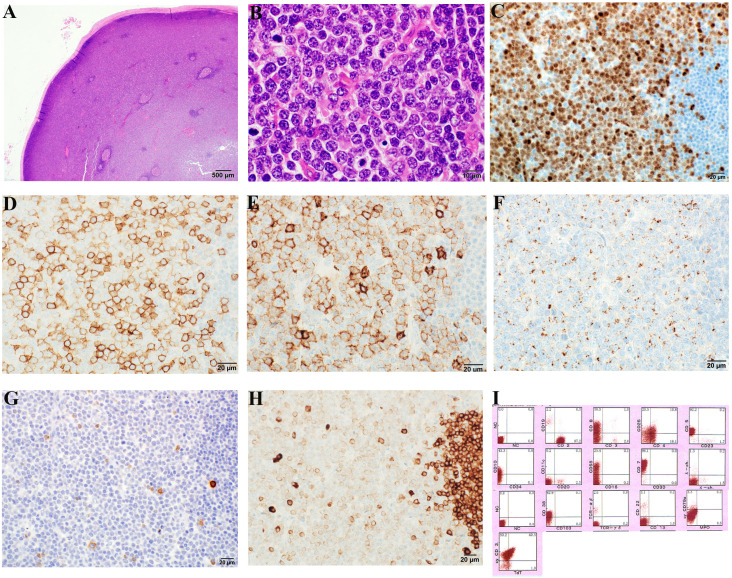
急性 T 淋巴细胞白血病/淋巴瘤(NOS)(T-ALL/LBL)和外周 T 细胞淋巴瘤(PTCL)同时出现的情况并不多见,只有少数几个病例同时出现。在这些病例中,PTCL 是在原发性 T-ALL 治疗后复发的,属于罕见的γ/δ型,T-ALL/LBL 病例中很少累及皮肤。我们在此报告了第一例在初治前同时伴有皮肤γ/δ型PTCL的新发T-LBL病例。一名70岁的男性患者出现全身淋巴结病变。淋巴结活检发现大量淋巴母细胞增生;免疫组化显示,这些细胞的TdT/CD1a/CD99、细胞质CD3ε、CD4和CD8阳性,T细胞受体(TCR)βf-1阴性。少数TCRδ阳性细胞夹杂其中。异常的是,TIA呈局灶性阳性,而颗粒酶/穿孔素呈阴性。在开始治疗T-LBL之前,躯干上出现了多个丘疹和斑块。皮肤活检发现大量增生的中型到大型非典型淋巴细胞,它们是TdT/CD1a阴性的成熟T细胞;TCRβf1和CD4阴性,TCRδ、CD5、CD8、CD56、TIA、颗粒酶B和穿孔素阳性。对 TCRG 的常规 PCR 分析显示,两个肿瘤之间没有相同的克隆带。皮肤病变被诊断为皮肤γ/δT细胞淋巴瘤。病变是原发性还是T-LBL的转化尚不清楚。在使用针对T-LBL的减量高CVAD/MA治疗后,患者获得了分子完全缓解。当T-ALL/LBL病程中出现不常见的皮肤病变时,无论是新发还是复发,都需要进行病理和遗传学评估,并假定可能同时存在γ/δ PTCL。
Coincidence of de novo T-lymphoblastic lymphoma and cutaneous gamma/delta peripheral T-cell lymphoma.
The coincidence of acute T-lymphoblastic leukemia/lymphoma, NOS (T-ALL/LBL), and peripheral T-cell lymphoma (PTCL) is unusual, and there have only been a few cases of their metachronous occurrence. In these cases, PTCLs emerged as recurrence after primary therapy for primary T-ALL, were the rare gamma/delta type, and uncommonly involved skin for T-ALL/LBL. We herein report the first case of de novo T-LBL that coincided with cutaneous gamma/delta PTCL before primary therapy. A 70-year-old man presented with systemic lymphadenopathy. Lymph node biopsy revealed a massive proliferation of lymphoblastoid cells; immunohistochemically, they were positive for TdT/CD1a/CD99, and cytoplasmic CD3ε, CD4, and CD8 and were negative for T-cell receptor (TCR) βf-1. A few TCRδ-positive cells were intermingled. Atypically, TIA was focally positive, whereas granzyme/perforin was negative. Multiple papules and plaques emerged on the trunk before the initiation of treatment for T-LBL. Skin biopsy revealed a massive proliferation of medium-to-large atypical lymphoid cells that were TdT/CD1a-negative mature T-cells; they were negative for TCRβf1 and CD4, and positive for TCRδ, CD5, CD8, CD56, TIA, granzyme B, and perforin. A conventional PCR analysis of TCRG showed no identical clonal band between the two tumors. The skin lesion was diagnosed as cutaneous gamma/delta T-cell lymphoma. Whether the lesion was primary or a transformation of T-LBL was unclear. After treating with reduced hyper-CVAD/MA targeting T-LBL, molecular complete remission was achieved. When an uncommon cutaneous lesion emerges in the course of T-ALL/LBL, both need to be evaluated pathologically and genetically, whether de novo or recurrent, assuming the possibility of coincident gamma/delta PTCL.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
